Losing weight in your tongue probably isn't one of your New Year's resolutions. But maybe it should be if you have sleep apnea. MR images show that a slimmer tongue can reduce the severity of obstructive sleep apnea, according to a study published online January 10 in the American Journal of Respiratory and Critical Care Medicine.
Researchers from the University of Pennsylvania (UPenn) used MRI to see how weight loss correlated to reduction in the volume of fat in the tongue and oral structures in obese patients to lower their apnea-hypopnea index (AHI), which charts the number of obstructive sleep apnea events per hour.
"Most clinicians, and even experts in the sleep apnea world, have not typically focused on fat in the tongue for treating sleep apnea," said study co-author Dr. Richard Schwab, chief of UPenn's Sleep Center, in a statement. "Now that we know tongue fat is a risk factor and that sleep apnea improves when tongue fat is reduced, we have established a unique therapeutic target that we've never had before."
The current research follows a 2014 study by Schwab et al of obese patients with and without sleep apnea. The researchers at that time found that participants with sleep apnea had significantly larger tongues and a greater percentage of tongue fat compared with those without the condition.
In this follow-up study, Schwab and colleagues analyzed 67 obese participants (mean age, 49.4 ± 11.9 years) with a body mass index greater than 30 and mild to severe obstructive sleep apnea, with an AHI of more than 10 events per hour.
Participants underwent a 1.5-tesla MRI scan (Magnetom Espree, Siemens Healthineers) at the start of the study to gather baseline data, followed by a second MRI scan six months later. The researchers used the MR images to measure the size of the subjects' airways; soft-tissue volumes of the tongue, tongue fat, soft palate, and related areas; and their volume of abdominal fat. Statistical analyses, which included Pearson's correlations, then were performed to quantify overall weight loss and reductions to the volumes of the upper airway structures to determine which was most instrumental in reducing obstructive sleep apnea.
Overall, participants lost 9.5% (± 10.8%) of their body weight over the six-month period, which significantly reduced the number of sleep apnea events as measured by AHI by 30.7% (± 66.7%) (p = 0.0004). Subjects who lost at least 2.5% of their weight achieved a significant drop in AHI (23.3% ± 21.9%) (p < 0.0001).
Meanwhile, participants with no change in their overall weight failed to change their AHI significantly (p = 0.856).
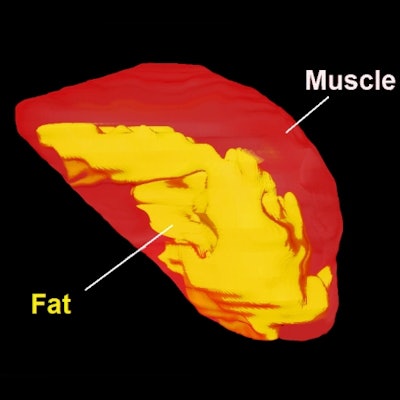
 Three-dimensional reconstruction of tongue (red) and tongue fat (yellow) derived from axial MRI and Dixon fat-only MRI show the loss of tongue fat between baseline and six-month follow-up in the same male patient. Images courtesy of American Journal of Respiratory and Critical Care Medicine.
Three-dimensional reconstruction of tongue (red) and tongue fat (yellow) derived from axial MRI and Dixon fat-only MRI show the loss of tongue fat between baseline and six-month follow-up in the same male patient. Images courtesy of American Journal of Respiratory and Critical Care Medicine.Most importantly, weight loss was significantly associated with reduced tongue fat volume, pterygoid volume (the jaw muscle that controls chewing), and total lateral wall volume (the muscles on the sides of the airway). Concurrently, the greater percentage decreases in tongue fat volume were associated with larger reductions in AHI (0.62, p < 0.0001). This finding "remained nominally significant also controlling for weight change," the authors added, "suggesting reduced tongue fat is independently associated with reduced AHI."



















