In a proof-of-concept study with phantoms, researchers were able to demonstrate that a dynamic chest radiography protocol was able to detect lung tumor invasion, according to findings published February 3 in Medical Physics.
Researchers from Japan and the U.S. showed that their dynamic chest radiography (DCR) technique produced bone-suppression images that enabled motion analysis of lung tumors, and at a radiation dose equivalent to conventional chest x-ray (Medical Physics, February 2021). They believe the technique could provide an alternative to chest CT for preoperative imaging.
In their introduction, the authors note that preoperative assessment of tumor invasion and adhesion is key when planning surgical excision of lung tumors. If the tumor moves independent of parietal or mediastinal pleura, it means that the tumor is not invasive or strongly adheres to lung tissue, and therefore may be easier to remove surgically.
Imaging modalities like cine MRI or breathing chest CT can be used to assess tumor invasion and adhesion. But both are more costly than x-ray; MRI often isn't available, while CT carries a higher radiation burden than radiography.
Dynamic chest radiography could be considered as an alternative, performed as a supplement to chest radiography using a dynamic flat-panel digital detector in a general x-ray room, wrote a team led by Rie Tanaka, PhD, of Kanazawa University in Japan. With DCR, a series of sequential chest radiographs are obtained of a standing patient through a 10-second respiratory cycle. Except for the breathing pattern, images are acquired in the same manner as a conventional radiograph.
A previous study published in April 2020 in Radiology Case Reports found that dynamic chest radiography was feasible for assessing tumor invasion preoperatively, but that overlying rib shadows and a lack of 3D visualization inhibited its quantitative performance. The use of bone suppression image processing could overcome this limitation, however.
Therefore, Tanaka et al decided to test the ability of dynamic chest radiography with bone suppression image processing applied to perform quantitative assessment of the adhesion of lung tumors. They based their study on imaging of an XCAT phantom that could simulate the presence of lung tumors with and without invasion; tumor motion could be simulated without the need to irradiate patients.
To simulate a solid tumor, the researchers created 30-mm tumor spheres and inserted them into each lung lobe of a virtual patient. Three types of tumor conditions were simulated, ranging from involving the chest wall or aorta to a location away from these structures. A total of 18 tumors were created, six with invasion and 12 without.
Image acquisition was simulated with software set to model a dynamic flat-panel detector x-ray system, and bone suppression was applied to resulting projection images that consisted of 150 respiratory phases of 10 seconds each.
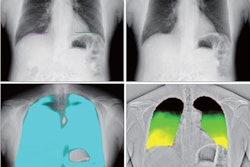
The movement of tumors in the phantom was analyzed quantitatively and calculated using five metrics originally derived from 4D ventilation-dynamic CT studies of lung tumor motion. Tanaka and colleagues wrote that motion tracking functioned properly on bone suppression images but was disrupted by rib shadows on images without the image processing.
The researchers found that dynamic chest radiography was able to discern the difference between lung tumors with and without invasion using the five quantitative metrics that measured tumor movement. They also found that bone suppression image processing worked well for providing precise motion tracking of lung tumors, but since the images in the study images were simulated, the technique might require further study before application in a clinical study.
Additionally, the authors noted several other technical issues with the technique, mostly related to the presentation and movement of tumors in different areas of the lungs, such as in the upper lobe and behind the heart. They also recommend the investigation of dynamic chest radiography in patients of different physiques, as well as with tumors of different sizes, shapes, and composition.
On the positive side, the radiation dose of the technique was just 1.9 mGy, the recommended level for a standard posterior-anterior chest radiograph.
In the end, Tanaka et al noted that dynamic chest radiography can distinguish between tumors with and without pleural invasion and adhesion using their quantitative analysis technique performed during patient respiration. Bone suppression image processing improves its performance, but additional image processing may be needed for tumors in certain areas.