Spectral CT has much to offer radiology. Also known as dual-energy CT (DECT), the technology gives radiologists the ability to more easily differentiate healthy from diseased tissue. And through careful planning, imaging facilities optimize their use of spectral CT to the benefit of patients and referring physicians.
Spectral CT isn't without its challenges, however. The workflow of dual-energy imaging can be more complex than conventional CT, and the technology generates greater volumes of data. But these are all challenges that can be overcome, according to several sources.
The keys are to optimize spectral CT protocols and have a champion who can shepherd the process. Alternatively, spend time at an institution that has extensive experience with the machine, the sources said.
Make it a team effort
How is spectral CT different from conventional CT? By scanning at two different x-ray energy levels, spectral CT can provide crucial information on the nature of tissues based on how they respond to the different x-ray beams. (Read more about the clinical advantages of spectral CT.)
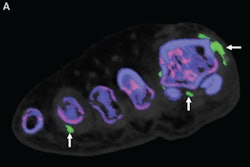
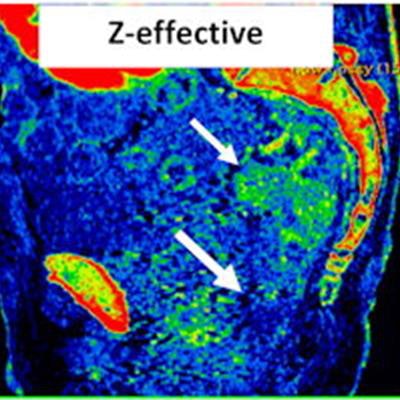
 Sagittal pelvis spectral CT scan of 65-year-old man with rectal adenocarcinoma. Conventional CT scan shows apparent hyperenhancing tumor that extends from the midrectum (small arrow) to the distal rectum (large arrow). However, the iodine map reveals iodine enhancement only involves the midrectum and spares the distal rectum. The water map confirms that the hyperdensity of the distal rectum is due to noniodine-containing radiodense stool. The z-effective image further shows that enhancing tumor only involves the midrectum and not the distal rectum. This case illustrates the value of spectral CT over regular CT to improve clinical tumor staging by differentiating between ambiguous densities. Image courtesy of Dr. Benjamin Yeh.
Sagittal pelvis spectral CT scan of 65-year-old man with rectal adenocarcinoma. Conventional CT scan shows apparent hyperenhancing tumor that extends from the midrectum (small arrow) to the distal rectum (large arrow). However, the iodine map reveals iodine enhancement only involves the midrectum and spares the distal rectum. The water map confirms that the hyperdensity of the distal rectum is due to noniodine-containing radiodense stool. The z-effective image further shows that enhancing tumor only involves the midrectum and not the distal rectum. This case illustrates the value of spectral CT over regular CT to improve clinical tumor staging by differentiating between ambiguous densities. Image courtesy of Dr. Benjamin Yeh.Another difference is that practices must think about the implementation of spectral CT prospectively, according to Dr. Achille Mileto, a senior associate consultant at the Mayo Clinic in Rochester, MN. It's more complex than just swapping a new CT scanner into an existing room.
 Dr. Achille Mileto of the Mayo Clinic in Rochester, MN.
Dr. Achille Mileto of the Mayo Clinic in Rochester, MN."It's a multistep implementation and integration process from the initial purchase to the moment of reading the clinical scans," he said. "This is not a 'plug-and-play' type of thing. It requires multiple iterations and coordinated team efforts of optimization."
Mileto and others emphasized the importance of collaboration when it comes to implementing spectral CT. Practices need a team of experts -- physicians, physicists, vendor application specialists, and departmental IT services -- to work together from start to finish.
"If you have a physicist, spend some time together and talk through what the issues are. What are the things we can work on optimizing? And then implement those solutions," said Tim Szczykutowicz, PhD, an associate professor of medical physics, radiology, and biomedical engineering at the University of Wisconsin-Madison.
Because spectral CT produces so many images, it's important for radiologic technologists to know which images the radiologist actually wants, he added.
 Tim Szczykutowicz, PhD. University of Wisconsin-Madison.
Tim Szczykutowicz, PhD. University of Wisconsin-Madison."Even at my academic university, when we roll out a dual-energy protocol, we'll get radiologists who ... if they weren't involved with why we picked the images we picked, will complain and say, 'What are all these extra images?' " Szczykutowicz said. "And even if one group of people thoughtfully picked the best images we need with spectral CT, if everyone wasn't in that discussion, and they don't think they need [those images], you've got a change management problem."
It can help to get everyone involved in spectral CT as early as possible. If that happens, working with spectral CT can be smooth sailing, as evidenced by the experience of Dr. Alec Megibow, a radiology and surgery professor at NYU Grossman School of Medicine. His institution has used DECT since 2006, and he reads, on average, 45 scans a day.
"We've been doing this for 15 years, so I've adapted my abilities," he said. "It doesn't take me all that much longer [to read DECT images]. It takes me a little longer than if I didn't, but I keep in mind the patient. The patient to me is the most important person here."
Mileto echoed that sentiment. Spectral CT's clinical value to the patient should always be considered when debating the technology's worth.
"You can spend, let's say, a few extra minutes to look at additional images that come for free (no extra acquisition) with spectral CT or instead not use spectral CT, but that will come at the cost of not having additional information that may spare an extra scan to the patient," he said. "It's a balance. If you use spectral CT in a nonoptimized way, you may have up to an extra thousand images coming to PACS, and if you're concerned about looking at all the images for that exam, it may result in extra time. However, if you work in a practice that strongly believes in protocol optimization, you may not have to deal with that many extra images."
What about the extra images?
It's true that spectral CT generates more images than conventional CT, but that again underscores the need for protocol optimization and discerning which images are crucial for each case. Spectral CT is capable of generating a lot of information, but not all of that information is useful all of the time.
"Some radiologist at the end of the day is going to open a study and see four more image volumes and ask, 'What am I supposed to do with these? Which one is really key here? Do I have to look at all of them?' " Szczykutowicz said.
The short answer is no; the radiologist doesn't need to look at every image spectral CT generates.
"You don't need to view those images to make diagnoses in the vast majority of cases," Megibow noted.
The spectral CT images only come into play with about 10% of cases, such as renal cases, and with those, Megibow is strategic, looking at the compressed images with the understanding he has the thin sections to go back to within the workstation.
"We look at every image," he said. "But we look at each in a way that allows us to get through the day."
Knowing which images to interpret -- and when -- is a critical strategy in overcoming workflow challenges. Ideally, a champion is onsite to help guide the process. Alternatively, spectral CT users can consult with vendors, some of which offer consultation programs for radiologists to shadow physicians and technologists who use spectral CT with ease.
Another important strategy to adopting spectral CT is to bear in mind it's a different beast than conventional CT.
 Dr. Benjamin Yeh of the University of California, San Francisco.
Dr. Benjamin Yeh of the University of California, San Francisco."For many years, radiologists thought about CT as a monoparametric technique -- very simple, based on Hounsfield units, and viewable in the axial, sagittal, and coronal planes," Mileto said. "Spectral CT exams come with low keV series, high keV images, an iodine map, virtual unenhanced images, calcium images; it's more complex with more images coming to PACS, and we, as radiologists, feel compelled to look at every image series made available. We were accustomed to the simplicity of CT, whereas dual-energy CT techniques add a multiparametric component that could be compared, to some extent, with MR."
In reality, however, these reconstructions are not like MRI, in which the image is a brand-new reconstruction, according to Dr. Benjamin Yeh, a radiology and biomedical imaging professor at the University of California, San Francisco.
"These images are just versions of the original dual-energy CT data," he said. "It should be more like window leveling for CT. It should be something you do on the fly as you need it rather than clutter up the entire screen with additional series because most of the time you don't need them."
The final word
While many of the traditional workflow challenges that spectral CT poses are being solved, users still would like to see more of a plug-and-play environment between different vendors, particularly between hardware and software from different companies. Often, data generated by a spectral CT scanner doesn't play well if it's viewed on a different vendor's software, Yeh explained.
The current solution is to create the images the radiologist would like to view for each vendor and then send the three or four additional views to PACS so there are three or four extra series of images for each scan, according to Yeh.
"That can be very confusing to radiologists, and it's inconvenient," he said. "It's tough because of how hardwired the images are to specific vendors and their own reconstruction software. Breakthroughs will have to come through vendors or the PACS units."
Mileto agrees that the DECT vendors need to work together more, including with PACS vendors.
 Peter Noël, PhD. University of Pennsylvania.
Peter Noël, PhD. University of Pennsylvania."In terms of solving some of the workflow challenges of spectral CT, the example that I like to give is to think about when radiologists used to print a number of different films to resolve images with soft-tissue window, lung window, and bone window," he explained. "With PACS, now you can move between different windows by pushing a button on the computer keyboard. Maybe in the coming future, we will be able to integrate the wealth of information provided by spectral CT in the same way. Key for this to happen will be to have radiologists, CT, and PACS vendors work together more."
Peter Noël, PhD, an assistant radiology professor at the University of Pennsylvania, is optimistic about the future of spectral CT.
"My prediction, and I'm very certain about it, is that a couple of years from now, you won't be able to buy conventional CTs anymore," he said. "So every CT we buy will be spectral, and this will automatically change the way people will work."