Shear-wave elastography (SWE) of the liver can help avoid invasive procedures such as liver biopsies, but proper execution is paramount. How can radiologists make sure they're imaging the liver effectively using SWE?
 Dr. Giovanna Ferraioli.
Dr. Giovanna Ferraioli.Shear-wave elastography is an ultrasound technique that assesses liver stiffness in diffuse liver disease by generating shear waves via tissue compression. Shear waves can be produced by external compression on the skin using a dedicated device or by using the force of the ultrasound beam applied directly into the body, according to Dr. Giovanna Ferraioli from the Medical School University of Pavia in Pavia, Italy. Ferraioli was first author on a recent article published in Medical Ultrasonography that offers tips for effective SWE imaging.
When shear waves are generated by a body-surface vibration, it's known as vibration-controlled transient elastography (VCTE). The vibration frequency is controlled (50 Hz), and so are its shape and amplitude.
When shear waves are generated by the push-pulse of a focused ultrasound beam directly in the tissue, it's called acoustic radiation force impulse (ARFI). A convex or linear transducer transmits focused ultrasound pulses that are repeated several times in a short stint. B-mode tracking pulses detect the propagation velocity of the shear wave by measuring the difference in arrival time (time lag) between two points at known distances apart from each other, according to the article.
"ARFI-based techniques can be used for assessing the stiffness of other organs as well; however, the best application where shear-wave elastography can be considered a real breakthrough is for the noninvasive staging of liver fibrosis," Ferraioli said in an interview. "The deformation arising from tissue compression propagates laterally -- it's like when a stone is thrown in water and you see all waves. The speed of the propagation is directly related to tissue stiffness: The stiffer the tissue, the higher the speed. The speed can be converted in the measure of stiffness (kPa) using the Young's modulus and assuming that the tissue is purely elastic."
Shear-wave speed is nearly 1,000 times less than ultrasound velocity in soft tissue, with shear waves attenuating swiftly, whereas some do not propagate in simple fluids at all. Also, shear waves propagate faster in stiffer tissue than in softer tissue, a phenomenon that forms the basis for using SWE to differentiate between tissue types.
In terms of the liver specifically, stiffness directly correlates with degree of fibrosis and indirectly with portal hypertension. Stiffness also corresponds with the risk of developing hepatocellular carcinoma (HCC).
Don't use SWE to differentiate between benign and malignant lesions, but do use it to rule out compensated advanced chronic liver disease (cACLD) and cirrhosis, and also as a first-line assessment for liver fibrosis severity. For both VCTE and ARFI-based techniques, the consensus is that values ≤ 5 kPa (1.3 m/s) have a high probability of being normal.
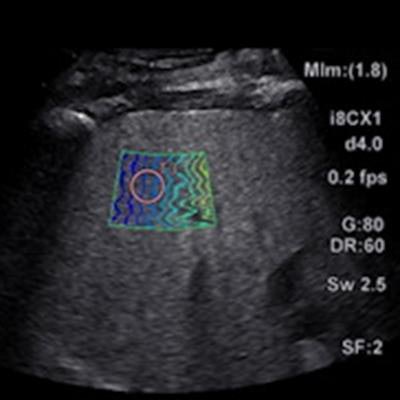
 A 60-year-old woman with nonalcoholic fatty liver disease. Liver stiffness one year prior was 5 kPa (1.3 m/s). Image courtesy of Dr. Richard Barr.
A 60-year-old woman with nonalcoholic fatty liver disease. Liver stiffness one year prior was 5 kPa (1.3 m/s). Image courtesy of Dr. Richard Barr. A 63-year-old man with a fatty liver and normal liver enzymes. Image courtesy of Dr. Richard Barr.
A 63-year-old man with a fatty liver and normal liver enzymes. Image courtesy of Dr. Richard Barr.Tips for using SWE
For most effective use of SWE, the ultrasound transducer should be positioned in an intercostal space -- perpendicular to the liver in both superior/inferior and right/left planes. The transducer's position can be assessed by looking at the liver capsule that appears as a sharp white line, parallel to the transducer's line, the authors said.
Also, be sure to avoid the ribs or the lung artifacts and note the quality of the B-mode image affects the quality of the SWE acquisitions. Common limitations such as poor acoustic window, limited penetration, and rib or lung shadowing can influence the feasibility and the performance of SWE. However, some of these limitations can be avoided.
Patients should breathe normally while the sonographer is searching for the best acoustic window and best area of liver parenchyma. However, before acquiring the SWE image, the sonographer should ask the patient to hold their breath in a neutral position without performing a Valsalva's maneuver. Measurements should be performed at least 1-2 cm below the liver capsule to avoid reverberation artifacts, the authors added.
 Dr. Richard Barr.
Dr. Richard Barr.This may sound complicated, and for that reason, article co-author Dr. Richard Barr, of Northeastern Ohio Medical University in Rootstown, OH, advises that sonographers receive hands-on training.
"It's obvious sometimes when you explain to people what to do that they may not completely understand what you're saying," he said. "It's really important to have hands-on training, have somebody watch you and tell you what you're doing wrong and help you through the process."
There are some additional considerations to note for SWE. For instance, due to the attenuation of the ultrasound beam, going deeper than 7 cm in most systems is problematic as deeper measurements have a lower signal/noise ratio. At the same time, deep abdominal probes allow for greater depth in higher body mass index patients.
"The problem is even though we're using the probe at the upper limits of what the FDA [U.S. Food and Drug Administration] requires, if you're going through a liver, particularly if it's a fatty liver, or a very stiff liver from fibrosis, that ARFI pulse is attenuated," Barr said. "And as it goes deeper and deeper in the liver, it becomes weaker and weaker. We get to the point where we don't really generate shear waves that we can measure and this is kind of the biggest problem we have. In North America, we've got people that are pretty big, and in those big patients, particularly if they have a really fatty liver or they've got a lot of subcutaneous fat, that weakens those pulses."
Other confounding factors occur when patients eat prior to the exam, or drink alcohol in general. Eating may increase the stiffness of the liver, so it's best to perform SWE when the patient has fasted for at least four hours, the article authors said. In terms of alcohol, abstinence altogether produces the best results.
"Alcohol ingestion is a huge, huge problem," Barr said. "It creates an enormous amount of inflammation in the liver and these people can have very high liver stiffness values, but maybe not so much fibrosis. Really, we need to have that patient almost abstain from alcohol for maybe a month to be able to get a measurement that really reflects the true degree of fibrosis."
It's confusing because as Barr mentioned, liver stiffness does not necessarily mean liver fibrosis. However, stiffness can reflect other physiological or pathological conditions such as hepatic inflammation, obstructive cholestasis, neoplastic and other infiltration of the liver, and hepatic congestion.
"Liver stiffness correlates directly with liver fibrosis once confounding factors are excluded," Ferraioli noted.
Worth the challenges
But despite its challenges, there are major benefits to shear-wave elastography for liver imaging. Determining liver fibrosis in a noninvasive way means the number of liver biopsies has nosedived.
"Since the beginning of this year at the university hospital where I work, very few liver biopsies have been performed," Ferraioli said. "In the past, when shear-wave elastography was not available, we performed some 200 liver biopsies per year. The number of liver biopsies has decreased not only in our hospital, but also all over Italy, Europe, and the world."
Despite its recent growth, Ferraioli believes that shear-wave elastography still hasn't achieved its full potential yet.
"We are assessing elasticity of a tissue, but tissue is not only elastic, it's also viscous," she said. "Viscosity may affect the stiffness value. Nowadays there's a possibility to assess, to do research and focus on viscosity. In the future we may have a tool that combines viscosity and elasticity and gives more accurate information."