High barium doses aren't necessary for reduced-prep virtual colonoscopy when a low-residue diet is part of the protocol. In the American Journal of Roentgenology, researchers from Belgium reported high sensitivity and specificity for colorectal polyps using such a protocol.
"Reducing the cathartic preparation is invaluable to improve patient compliance because the latter is related to the success of a screening program," wrote Drs. Philippe Lefere, Stefaan Gryspeerdt, Jesse Marrannes, and colleagues from Stedelijk Ziekenhuis in Roeselare, Belgium (AJR, June 2005, Vol. 184:6, pp. 1836-1842).
The study aimed to evaluate dietary fecal tagging for virtual colonoscopy using only 50 mL of a 40% weight/volume barium suspension (Tagitol V, E-Z-EM, Lake Success, NY) taken with meals for two days before VC. The cohort of 200 subjects 50 years and older included 63 with a history of previous polypectomy or colorectal cancer, 29 with a family history of colorectal lesions of cancer before age 60, nine with a positive fecal-occult blood test, and 17 who were unwilling to undergo conventional colonoscopy, among others.
"The patients were asked to avoid food rich in fiber or pulp: flavored cheese, condiments, whole-grain bread, crackers, cereal, popcorn, raw fruit, mustard, jam, and garlic," the authors wrote. The day before the exam they received commercially available low-residue meal kits (NutraPrep, E-Z-EM) consisting of powdered drinks, orange juice, soups, nutrition bars, crackers, and apple sauce.
The reduced cathartic cleansing regimen included 16.5 mg of magnesium citrate followed by four bisacodyl tablets the evening before VC.
The day of the exam, 125 patients were scanned using a single-detector scanner (Tomoscan AV/EU, Philips Medical Systems, Andover, MA) with 5-mm slice thickness, 7-mm table feed, pitch 1, and 2-mm slice reconstructions. Another 85 patients were imaged on a multidetector scanner (HiSpeed, GE Healthcare, Chalfont St. Giles, U.K.) using 2.5-mm collimation, 120 kVp, 70 mAs, pitch 1.35, and 0.6-sec gantry rotation.
All patients received 20 mg of hyoscine butylbromide (Buscopan, Boehringer Ingelheim, Ingelheim, Germany) as an antispasmodic, followed by colonic insufflation with CO2 using an automated device (ProtoCO2l, E-Z-EM). Follow-up with conventional colonoscopy (n = 42) or an additional VC exam served as the gold standard in some cases. Not having every case controlled by conventional colonoscopy represents an important study limitation, the authors noted.
The team assessed colonic distension in every patient on the scout view, and the colon was evaluated by segment and by patient using an InnerView GI workstation (E-Z-EM) equipped with endoluminal software that was used to examine the data with 2D primarily, with 3D problem-solving, the authors wrote.
In all, 1,200 segments were evaluated by segment and by patient, and measured on magnified CT images using a caliper. The efficacy of tagging in feces 6 mm and larger was inspected visually, and deemed tagged or nontagged. The smaller feces were not inspected in this manner, considering that diminutive lesions of this size can also be safely ignored.
 |
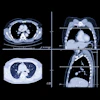
| Above: Supine image of rectum in a 64-year-old woman shows nontagged material 6 mm or greater with small hyperdense spot in dependent part of rectum (arrow). Hyperdense spot probably corresponds to some barium. Below: Prone view of rectum in the same patient shows nontagged fecal material has moved to anterior rectal wall (arrow). Image shows nontagged feces 6 mm or larger in rectum, possibly caused by remnants of bisacodyl suppository. P Lefere, S Gryspeerdt, J Marrannes, M Baekelandt, B Van Holsbeeck, "CT Colonography After Fecal Tagging with a Reduced Cathartic Cleansing and a Reduced Volume of Barium" (AJR 2005, 184: 1836-1842). |
 |
Overall the researchers found residual feces in 413 segments (34.41%), including fecal material smaller than 6 mm in 210 segments (17.5%) and 6 mm or larger in 203 segments (16.92%). In addition, 527 segments contained residual fluid (43.91%), detected as it moved between prone and supine imaging. Nontagged feces 6 mm or greater were present in 49 segments (4.08%) and nontagged fluid in 178 segments (14.83%).
A total of 65 lesions 6 mm or larger were correctly diagnosed using primary VC, producing six false positives in five patients, the authors wrote. In two patients, two lesions adjacent to each other were misinterpreted as being only one. Another 8-mm lesion was missed, and an additional polypoid lesion was found only in the prone data, and also detected on conventional colonoscopy.
Conventional colonoscopy found 68 lesions, including 13 hyperplastic polyps, 44 adenomatous polyps (five with severe dysplasia), and 11 adenocarcinomas, four presenting as a stenosing apple-core lesions.
"The false positives were caused in four patients because of diverticulosis with severe luminal narrowing and thickening of the folds," Lefere and colleagues commented. In these cases, a differential diagnosis that included carcinoma was made. Only 4% of segments presented with untagged feces 6 mm or larger, and this result was limited to the presence of one fecal ball in more than two-thirds of these patients.
"The good results of tagging are reflected in the results of polyp detection," Lefere and colleagues wrote. "In fact, there were no false-positive findings caused by nontagged feces. Three false negatives of a total of 68 lesions 6 mm or greater were reported. Only one lesion of 6 mm or greater was overlooked, and it was detected retrospectively. The two other lesions were adjacent to another lesion and were hence misinterpreted as being a bilobulate rather as being two separate lesions."
The protocol also remained robust in a wide range of patients, including eight with a stenosing adenocarcinoma, "representing a possible burden for colonic preparation or tagging," they added. But only one of these patients had more fecal residue than average, and the prep failed in only two patients who admitted that their compliance had been incomplete, according to the authors.
"These cases underscore the importance of providing detailed instructions to the patients," they wrote. In some cases poor tagging may have resulted from the patient's drinking too much regular fluid the day before or the morning of their VC exams, as evidenced by the location of the nontagged fluid.
"In 64.5% of patients with nontagged fluid, there was nontagged fluid in both the right hemicolon and the small bowel," the group wrote. "It is also clear that dietary fecal tagging could still be improved by adjusting the barium regimen."
The results using only 50 mL of a 40% w/v barium suspension are promising, they wrote. "Further research is needed to optimize fluid tagging to enable fecal subtraction and a primary 3D read."
By Eric Barnes
AuntMinnie.com staff writer
July 13, 2005
Related Reading
Prepless VC yields high sensitivity in average-risk subjects, June 10, 2005
CAD struggles through tagged, subtracted VC data, May 18, 2005
Iodine tagging regimen yields best VC results, January 27, 2005
Low-prep VC study finds CAD can be fooled, December 23, 2004
Ultralow-dose virtual colonoscopy shows high sensitivity, April 8, 2003
Copyright © 2005 AuntMinnie.com