Prototype colon CAD systems are proliferating, and thanks to years of painstaking development work they're doing a pretty good job, outperforming all but the best radiologists in the detection of colonic lesions.
But even as developers strive for regulatory approval and eventual commercialization of their systems, colon CAD faces important technical challenges that have arisen not only from the sheer difficulty of finding polyps, but also from today's increasingly patient-friendly but radiologist-confounding VC protocols, which emphasize low-dose image acquisition and minimal bowel preparation.
In a talk at the 2005 Computer Assisted Radiology and Surgery (CARS) meeting in Berlin, VC CAD expert Dr. Hiro Yoshida from Harvard Medical School in Boston discussed the major innovations that have produced today's complex CAD systems, and the moving target CAD developers face in keeping up with new performance standards.
Challenges or no, CAD remains a hot commodity that everyone seems to want a piece of.
"If you look at the literature, several CAD systems already have been reported for the detection of polyps during last five years," Yoshida said. "Seven academic institutions are now working on it, and at least five commercial companies are rushing to make a business out of it."
How they work
CAD's first job is to segment the colon. This step serves to limit the search area for polyps to reduce primary processing time, "and also sometimes to reduce causes of false positives coming from the small bowel and extracolonic structures," Yoshida said.
To segment the colon, CAD schemes rely a priori on differences in CT attenuation values. Isotropic volumes are generated by interpolation of the CT data, and anatomy-based extraction processes are then used to analyze a histogram of CT values, he said.
Yet segmentation is never perfect, as it often segments bits of fecal material or small-bowel data along with the colon. As a result, researchers have labored to design algorithms that segment the colon efficiently while minimizing shortcomings. Important developments in segmentation include:
Vector quantization (Chen et al, IEEE Transactions on Medical Imaging, December 2000, Vol. 19:12, pp. 1220-1226) -- This multistage technique uses modified self-adaptive online vector quantization for low-level image classification, as well as a region-growing strategy for high-level feature extraction.
Distance transform (Wyatt et al, Computerized Medical Imaging & Graphics, January-February 2000, Vol. 24:1, pp. 1-9) -- To automate the colon segmentation process, this group developed a method of locating seed points and segmenting gas-filled lumen sections without user supervision.
Knowledge-based segmentation (Nappi, Yoshida et al, July-August 2002, Journal of Computer Assisted Tomography, Vol. 26:4, pp. 493-504) -- The University of Chicago team improved its previous anatomy-oriented colon segmentation technique with a colon-based analysis step that performs self-adjusting volume-growing within the colonic lumen, and traces the air-filled regions of the colon to remove the small bowel.
Multiple seed point placement (Iordanescu et al, Academic Radiology, February 2005, Vol. 12:2, pp. 182-190) -- This group's algorithm automatically locates seeds, or points for colon segmentation, in the cecum and rectum using 2D morphological operators to find pockets of colonic air.
Centerline-based segmentation (Frimmer, Yoshida et al, Medical Physics, in press, 2005) -- This method draws centerlines in the air-filled region in the colon, then intelligently connects these segments to extract the entire colon including collapsed colon segments.
Disconnected regions of the colon in CT data are due to collapsed colon segments resulting from myriad causes such as colon spasm, insufficient distension, occluding tumors, fluid and stool filling, and the like. Sometimes there are multiple causes of collapse, Yoshida said. Workarounds are possible, and efforts to intelligently connect disconnected segments are under way. But the results are always inferior to those obtained in clean, dry, distended colons, he said.
"Often what investigators do is to use anatomic knowledge to trace the internal lumen of the colon which is not connected by (air-filled regions) to the small bowel," Yoshida said. "Then we fill the collapsed segments out by region-growing and volume-growing in order to extract the entire colon."
Collapsed colons are hard to trace by any region-growing method, but succeeding in some measure is an important goal because extracolonic structures will always generate false-positive CAD results, while collapsed colons generate false negatives, he said. The centerline-based segmentation study in press (referenced above) was able to cover 96% of the colon while eliminating all but 1% of the extracolonic structures.
"But when you apply this kind of technique to a large number of colons, you see a trade-off between minimization of extracolonic structures, especially the small bowel, and maximizing the extracted colonic wall. And this trade-off is something you have to deal with when you design the algorithm," Yoshida said.
Electing polyp candidates
CAD's next job is to find polyp candidates that represent as many true polyps as possible without creating too many false positives. Developers have been fine-tuning their methods of performing this task for years.
"Most methods use shape analysis based on geometric features, wall thickness, volumetric shape index, sphere-fitting, or overlapping surface normal (method)," Yoshida said.
Polyp candidate segmentation is a polyp candidate detection method that works by measuring the volume and diameter of polyp candidates, and removing "outlier" data elements to enable quantitative visualization, he explained.
"If you identify these caplike structures, you are pinpointing the location of the polyp," Yoshida said. "After you find where the polyp is located, then you can do the region-growing or segmentation method of your choice in order to get the entire region of the polyp."
Two important polyp candidate segmentation methods are the conditional morphological dilation (Nappi et al, Medical Physics, January 2000, Vol. 30:7, pp. 1592-1601) and the fuzzy clustering/deformable model technique by Yao et al (IEEE Transactions on Medical Imaging, November 2004, Vol. 23:1, pp. 1344-1352).
"Most shape-based detection methods assume that the polyp is a polypoid lesion that protrudes sufficiently into the lumen," Yoshida said. "Therefore the most important sources of false negatives are diminutive polyps, especially less than 5 mm, or flat or depressed polyps."
Unfortunately, geometric-based polyp detection methods are poorly equipped to find flat lesions, he said, a shortcoming that will not be easily resolved.
Polyps that are inconspicuous due to imaging artifacts or obstructed by normal structures, and those that are invisible due to collapsed colon segments or fluid submersion, account for most other false negatives.
As for false positives, a 2002 study by Dr. Abraham Dachman, Yoshida, and colleagues at the University of Chicago found that 42% of false positives were generated by haustral folds or flexural pseudotumors. These causes were followed by stool (28%), small bowel and stomach data (9%), ileocecal valve (6%), motion artifact (3%), extrinsic compression (2%), rectal tube (2%), and other causes (9%).
 |
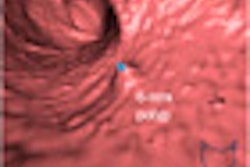
| Above, true polyps detected by the CAD algorithm. The three highlighted examples (lower right) were missed by the radiologist. |
Axing false positives
Once the polyp candidates have been assembled, the next task is, of course, to find, differentiate, and eliminate the false positives without eliminating true positives.
"Roughly speaking there are two approaches to dealing with false-positive reduction," Yoshida said. "One is the image feature-based approach, which characterizes false positives in the image's feature space and subjects those features into whatever classifiers you like. The second ... is a stool-mobility based approach."
Image feature-based classifiers work by analyzing structural features in the CT dataset such as folds and stool, and upon identifying them, eliminate them as nonpolyps based on a number of methods, including:
Edge displacement field (Acar et al, IEEE Transactions on Medical Imaging, December 2002, Vol. 21:12, pp. 1461-1467) -- The group's postprocessing technique models the way radiologists recognize polyps while scrolling a cross-sectional plane through 3D CT data by classifying changes in the location of the edges in the 2D plane.
Gradient concentration (Nappi, Yoshida et al, Academic Radiology, April 2002, Vol. 9:4, pp. 386-397) -- Gradient vectors at voxels in a polyp tend to point toward the center of the polyp because of its spherical shape, whereas those in a fold tend to converge to a line because of their elongated shape. Gradient concentration measures this concentration-pattern difference of the gradient vectors for differentiation between folds and polyps.
Curvature of the polyp neck (Jerebko et al, 2005. Academic Radiology, April 2005, Vol. 12:4, pp. 479-486) -- One distinctive polyp feature that helps to discriminate between true polyps and false positives is the curvature of the polyp neck, which is the average maximum principal curvature calculated around the neck circumference.
Classifiers for stool identification rely on textural analysis of internal patterns based on the fact that CT stool images tend to have a mottled pattern due to air bubbles and fat, Yoshida noted. Methods of stool detection have included:
CT attenuation (Summers et al, Radiology, April 2001, Vol. 219:1, pp. 51-59) -- In this method, the CT values of each voxel within a potential polyp are sampled along a single ray directed through the polyp to identify voxels that have soft-tissue attenuation within the potential polyp.
Random orthogonal shape section (Gokturk et al, IEEE Transactions on Medical Imaging, December 2001, Vol. 20:12, pp. 1251-1260) -- The random orthogonal shape sections method is a 3D pattern-processing technique that combines information from many random images to generate signatures of shape.
Volumetric texture analysis (Nappi, Yoshida, Academic Radiology, April 2002, Vol. 9:4, pp. 386-97) -- False positives due to stool are reduced by computing several 3D volumetric features that characterize the internal structures of the polyp candidates, and that distinguish between the mottle (stool) and a solid (polyp) textural pattern.
 |
| Segmented colon is subjected to CAD analysis and shown before (left) and after (right) false-positive reduction. All images courtesy of Dr. Hiro Yoshida. |
Yoshida and his colleagues have recently developed a stool mobility-based method of false-positive reduction, based on correspondence of supine and prone datasets.
The idea comes from standard VC practice: Polyps and stool that are very difficult to differentiate in either prone or supine views can often be distinguished if the finding moves between the prone and supine CT datasets, Yoshida said.
"Therefore, one approach is to divide the entire prone and supine dataset into different regions, and establish some region correspondence between them," he said. "Once you find some (CAD) detections ... then you attempt to find the corresponding detections in the other dataset. If there is no correspondence between supine and prone then you forget it -- because it's moved around so it's likely to be stool. And if it stays there then it's likely to be a polyp, so you keep it."
The team's preliminary study of 121 patients (242 datasets) achieved full or partial correspondence between prone and supine datasets in 71% of the cases. Overall, supine-prone correspondence eliminated 19% (73/365) of false positives without losing any true positives, Yoshida said (Nappi, Yoshida et al, Academic Radiology, June 2005, Vol. 12:6, pp. 695-707).
Classifiers
Investigators also use many different kinds of classifiers: for example, support vector machines (SVM) or classification and regression tree (CART) classifiers, to decide which features the above methods find in the data are likeliest to represent true polyps. Many kinds of feature classifiers have improved in recent years, Yoshida said, but selecting the best set of features to represent polyps remains difficult.
"There is a challenge as to which classifiers you want to select: parametric or nonparametric, supervised or unsupervised," he said. "After you choose a classifier then you have to choose a model in a classifier," or in other words, decide which parameter will work best for a particular classifier. VC classifiers have included:
Discriminant analysis (Yoshida, Nappi, IEEE Transactions on Medical Imaging, December 2001, Vol. 20:12, pp. 1261-1274) -- False-positive detections are reduced by computation of several 3D volumetric features characterizing the internal structures of the polyp candidates, followed by the application of discriminant analysis to the feature space generated by these volumetric features.
Support vector machines (Gokturk et al, 2001, previously cited) -- In this method, signatures obtained by means of the random orthogonal shape sections method are fed to a support vector machines technique for differentiation of false positives from polyps.
Classification and regression tree (Jerebko et al, Academic Radiology, February 2003, Vol. 10:2, pp. 154-160) -- The system involves classification by a committee of neural networks using distinct subsets of features including regional density, Gaussian, and mean curvature, as well as sphericity, lesion size, and colon wall thickness. Back-propagation neural networks trained with the Levenberg-Marquardt algorithm are used as primary classifiers, called committee members.
Committee bagging of artificial neural networks/support vector machines (Jerebko et al, previously cited) -- This group's CAD scheme uses a set of support vector machines for classification, a smoothed leave-one-out cross-validation method for obtaining error estimates, and a bootstrap aggregation method for training and model selection. Bagging, or bootstrap aggregation built on different feature subsets, is designed to improve classification performance compared with single support vector machines.
Bayesian artificial neural networks (Nappi, Yoshida et al, Proceedings of SPIE, February 2004, Vol. 5370, pp. 839-848) -- Bayesian artificial neural networks (BANN) learn from sample data like conventional neural networks. However, a BANN has the advantage of being able to simulate an "ideal reader" well, even when the training database is very limited in size. As a result, this method has been found empirically to perform better than other neural networks. Shape and texture features were calculated from the segmented polyps, and were subjected to a BANN to differentiate false positives from true polyps.
Once the CAD output is generated and the false positives reduced, the results must be integrated into the clinical workflow, and displayed on a user-friendly interface that integrates 2D and 3D data as seamlessly as possible, while highlighting the findings clearly. Such interfaces are being developed, of course.
"There's a chance that a truly sophisticated user interface including the likelihood of polyps would be more beneficial in colon CAD than in other modalities," Yoshida said.
CAD beats most radiologists
"When we superimpose sensitivity as a function of number of polyps along with human reader performance in untagged (VC), then you see that CAD results for sensitivity are at the higher end of human reader performance," Yoshida said. "Therefore, in terms of sensitivity, CAD has been doing a pretty good job."
 |
| CAD sensitivities are at the high end of reported human readers' sensitivities. |
 |
| False-positive rates of CAD systems tend to be much higher than those of human readers. |
Nevertheless, human readers overwhelmingly generate fewer false positives than CAD, he said.
Some people think this is not going to be a problem, given the time required for VC reading and the ease of dismissing the false-positives. Yoshida outlined a study presented by Dachman and colleagues at RSNA 2002 concluding that 88% (78/90) of false positives generated by CAD were easy to dismiss, while 13% (12/90) were difficult to dismiss (Radiology, 2002; 225(P): 303).
Still, even if only a few polyps are difficult to dismiss, those findings can be vexing. And because there is always some doubt about the accuracy of conventional colonoscopy as a reference standard, the findings could potentially be called incorrectly even when they are dismissed in the light of a negative conventional colonoscopy result.
"If you believe the colonoscopy reports, and if these are all false positives being wrongly identified by CAD as polyps, then the human readers may also identify these false positives as true polyps, which is one of the risks associated with having too many false positives generated from CAD," Yoshida said.
As for fecal tagging and electronic subtraction, these methods need further development and validation as well, he said.
"False negatives can happen because polyps can be partially covered by tagged stool, and because of partial-volume effects, tagging can brighten up the area and make it look like a tagged stool," Yoshida said. "Therefore, CAD gets rid of the polyp candidate in the middle of the process by wrongly identifying it as a piece of stool."
Room for improvement
The principal shortcoming of current CAD studies is their small size. Most CAD results were gleaned from datasets of fewer than 100 cases -- but a system can't really be validated thoroughly on fewer than 1,000 cases, he said.
But large VC databases are notoriously hard to come by. One possibility is the data acquired by Pickhardt and colleagues in the group's trial of 1,233 asymptomatic patients (New England Journal of Medicine, December 4, 2003, Vol. 349:23, pp. 2191-2200). And the National CT Colonography Trial (ACRIN Protocol 6664) will be another potential source.
In clinical practice, CAD's challenge is to substantially lower the false-positive rate while maintaining high sensitivity. Still, CAD schemes are known to generate lots of false positives from folds, stool, and extracolonic structures, Yoshida said.
"The fundamental scheme for CAD detection of polyps with CAD has been established. And many people are now getting on to serious clinical trials, including industry," he added.
In summary, CAD systems are improving rapidly, but daunting technical challenges remain, Yoshida said. Many more studies will be required to assess the effects of insufficient bowel preparation (intentional or otherwise), fecal tagging, inadequate bowel distension, and today's low-dose CT protocols.
By Eric Barnes
AuntMinnie.com staff writer
August 5, 2005
Related Reading
Part II: Computer-aided detection identifying new targets, July 15, 2005
Part I: Computer-aided detection marking new targets, July 14, 2005
VC CAD matches prone and supine imaging data, June 28, 2005
VC CAD shows progress toward clinical use, June 3, 2005
CAD struggles through tagged, subtracted VC data, May 18, 2005
Support vector machines boost accuracy of VC CAD, May 3, 2005
Copyright © 2005 AuntMinnie.com