No one wants to expose a child to radiation needlessly -- certainly not for cases in which ultrasound and MRI can provide a reliable diagnosis without the risks of ionizing radiation, which are substantially higher in younger patients.
But dose isn't the only concern in clinical practice. For cases in which high resolution and/or speed are paramount, some radiologists are finding MDCT to be the best alternative. And other modalities carry their own risks.
Close to 3 million CT examinations are performed annually on children in the U.S. According to the American Cancer Society, the use of CT in all populations has increased about sevenfold in the past 10 years.
An alternative imaging choice, MRI, has been getting faster, its resolution finer. Three-dimensional imaging software is coming into its own. MRI is the modality of choice for certain spine and brain applications, and, indeed, in many of the same soft-tissue imaging tasks where MRI excels in adults. One recent study, for example, found MRI to be far more sensitive and specific than high-resolution CT in diagnosing soft-tissue abnormalities of the inner ear prior to cochlear implantation (Otology & Neurotology, September 2005, Vol. 26:5, pp. 976-82).
Other researchers cite MRI's utility in pediatric tumor imaging, particularly when combined with new 3D software applications. MRI can determine the resectability of liver tumors; stage neuroblastoma in the bone marrow; image the lymph nodes, liver, and spinal canal; and evaluate Wilms' tumors preoperatively.
In an e-mail to AuntMinnie.com, Dr. Lars Thorelius, a radiologist from Linköping University Hospital in Sweden, made his case for the use of ultrasound in most pediatric applications, especially the abdomen.
"Go directly for CT in the absence of skilled sonologists, but if an experienced sonologist is available an ultrasound exam is the obvious first choice for kids' abdomens in most conditions," Thorelius wrote. "Add CT in the relatively few cases where ultrasound is not conclusive. This procedure does not have to delay the outcome: If in some hurry, begin oral CT contrast administration on the way to the ultrasound department, just in case. This 'beverage' often enhances ultrasound access. The experienced sonologist can work around gas and other obstacles in many cases. The clear correlation between the tender spot and the pathology is completely lost in other modalities...."
Of course, it's hard to beat MDCT in young lungs, where superior spatial and temporal resolution, along with speed and intrinsically high organ contrast, reveal exquisite anatomic detail. High-resolution chest CT scoring systems have been used in children to evaluate the extent and severity of cystic fibrosis, both in the airways and in lung parenchyma. In one study, CT measured air trapping in young patients with cystic fibrosis far more accurately than pulmonary function tests (Pediatric Pulmonology, November 2004, Vol. 38:5, pp. 396-405).
In noncystic-fibrosis-related bronchiectasis, MDCT showed a stronger correlation between the extent and severity of bronchiectasis and spirometry values than chest x-ray (Pediatric Pulmonology, August 2003, Vol. 36:2, pp. 87-93).
CT's advantages can be less clear-cut for routine imaging outside the lungs, for example in cardiac and vascular imaging, where ultrasound and MR are viable, radiation-free options at some facilities. Non-lung imaging in children was addressed in a presentation at the 2005 International Symposium on Multidetector-Row CT in San Francisco.
In his talk, Dr. S. Bruce Greenberg from Arkansas Children's Hospital in Little Rock and the University of Arkansas in Fayetteville offered his ideas on when to choose CT, MRI, or ultrasound.
A review of the logs at Greenberg's facility revealed that CT is most often deployed in children for trauma imaging; imaging of the head, temporal bones, sinuses, and orbits; body imaging for oncology and abdominal pain, skeletal anomalies, and cortical bone; and vascular imaging, Greenberg said.
In an example of a 6-year-old with congenital cholesteatoma, thin-section axial images (0.5-mm collimation) were acquired at 100 kVp and 100 mAs, and viewed on isovoxel coronal reconstructions.
 |
| Axial (left) and coronal (right) images of a 6-year-old with congenital cholesteatoma were acquired on a 16-slice MDCT scanner (Aquilion, Toshiba America Medical Systems, Tustin, CA) examined using isovoxel coronal reconstructions. All images courtesy of Dr. S. Bruce Greenberg. |
For sinus disease, Greenberg's group favors thin sections in a single plane (1-mm collimation, 80 kVp, 200 mAs) viewed on coronal reconstructions.
 |
| Axial (left) and coronal (right) images of a 3-year-old with right maxillary sinus disease. Axial 1-mm thick sections were acquired at 80 kVp and 200 mAs, and viewed using coronal reconstructions. |
 |
| Axial (left) and coronal (right) MDCT images of a 12-year-old with calcaneous osteoid osteoma show bone detail. |
MRA versus CTA
A principle area of uncertainty seems to be in vascular imaging, where MRA, CTA, and ultrasound all have their place, Greenberg said.
"It's an ongoing discussion at this point as to when to do CTA, when to do MRA in children," he said. "And the question really comes down to: Are we talking about radiation, or are we talking about sedation?"
CT's carries radiation risks down the road, of course, while the risk of sedation with MRA is more immediate. And risks associated with sedation are more variable, he said.
"When I talk about comparing the two in terms of risks, though, there's a geography of risks," Greenberg said. With CT, "a child receiving a rad (of radiation) in Minnesota is no different from a child receiving a rad in Mississippi," he said. "It's a very homogeneous kind of problem. However, when we talk about sedation risks it's local -- it's a heterogeneous problem."
Differences in sedation risk vary by institution, he said. Different facilities use different drug regimens, the people doing the sedation have varying levels of training, and the support structures are going to vary widely in the event something goes wrong.
"We've done tens of thousands of sedations in radiology department for children undergoing studies, and have had zero deaths," Greenberg said. "So the risk in the setting I'm in is very low. However, if someone is working, say, in an outpatient clinic or in a place where they perhaps don't do many children, then the risk of sedation may actually exceed the risk of radiation exposure."
Ultrasound is an important alternative for imaging vascular lesions, Greenberg said.
"(Ultrasound) has the appeal of no ionizing radiation, and with Doppler, of course, you can get some functional information as well," he said. Where you can use it I think it's the preferred approach -- it's probably underutilized." However, he said, ultrasound's limited field-of-view, as well as imaging limitations in the presence of gas or bone, can severely limit the overall utility of this modality.
CT is a good choice for general-purpose nonvascular imaging in cases in which MRA is unavailable, or when the radiation risk appears to be lower than the risk of sedation with MRA, he said. CT can also be used in cases in which MRA is contraindicated, and in cases of combined vascular and pulmonary disease.
"If you need higher spatial resolution than MRA will allow, or if you're dealing with a patient with metal stents or valves -- usually these are your congenital heart patient follow-ups -- I think CTA has a strong role," he said.
CT's higher spatial resolution was crucial in one example (a 7-year-old patient with right renal upper-pole pyelonephritis), due to the diminutive size of the affected structures, Greenberg said of an image displayed on the screen.
CT's speed relative to MRI also gives it the edge in trauma imaging, or when children are very sick, Greenberg said. He reinforced his point with a CT image of a 1-year-old trauma patient with a vertebral artery dissection.
 |
| MDCT spine images of a 1-year-old trauma patient show left vertebral artery dissection. |
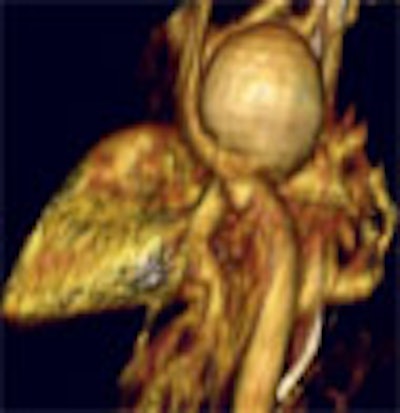
"Another child presented with pericarditis," Greenberg said. "But when the CT was done, we found this large ductal aneurysm which was filled with MRSA (methicillin-resistant staph aureus) -- certainly a child that you'd like to get in and out quickly."
 |
| In an infant presenting with pericarditis, MDCT showed a large mycotic aortic aneurysm. |
In a teenager with truncus arteriosis, CT showed calcification in the pulmonary artery conduit, and a prosthetic valve in the aorta.
"When we look at that valve a little more closely, the aorta above and the inflow below is bigger, so he's kind of outgrown the valve," Greenberg said. "There is an anomaly in the coronary arteries as well, in the form of a left main artery originating from the right coronary cusp." MRI would have been unable to depict all of the cardiac anomalies in the patient, he said.
"There are growing indications for MDCT in children," Greenberg concluded. "The isovoxel imaging, the multiplanar views, and 3D reconstructions for body imaging are being utilized just like in adults. I do believe that CTA will become and is becoming the dominant player for evaluating vasculature in infants and children. And I think the low-dose techniques being developed are very important for future growth in this area."
By Eric Barnes
AuntMinnie.com staff writer
September 30, 2005
Related Reading
Low-dose CT matches x-ray for pediatric sinus imaging, June 9, 2005
MDCT, MRI competitive in some bone lesion applications, June 20, 2005
Report finds vendors enable excess radiation doses in pediatric CR, DR, February 4, 2005
Use of pediatric head CT growing steadily in emergency departments, May 4, 2004
Constant image-noise standard lowers CT dose in pediatric exams, April 21, 2004
Copyright © 2005 AuntMinnie.com
















