The accurate diagnosis of gallbladder rupture with acute cholecystitis is key to arranging timely surgery and preventing serious outcomes. Acute cholecystitis, usually caused by a gallstone blocking the flow of bile, can be readily diagnosed in patients presenting with acute abdominal pain. Nevertheless, gallbladder rupture with many acute cases often goes undiagnosed until it's too late.
CT can close the gap and save lives by reliably detecting gallbladder ruptures presurgically if clinicians look for the signs, according to researchers from Taiwan who discussed their findings at the 2008 European Congress of Radiology (ECR) in Vienna.
"Gallbladder rupture is one of the most severe complications of acute cholecystitis," explained Dr. Jen-dar Chen from Taipei Veterans General Hospital and National Yang-Ming University School of Medicine, both in Taipei. "High morbidity and mortality are probably much worse than reported."
Early diagnosis and cholecystectomy are the gold standard for managing gallbladder rupture to avoid unsuccessful outcomes, he said. But while acute cholecystitis is well indicated by both clinical and imaging results, preoperative diagnosis of gallbladder rupture remains difficult.
"Most (ruptures) have only been diagnosed during surgery," Chen said.
To assess whether CT can reliably diagnose gallbladder rupture in acute cholecystitis cases, Chen and his colleagues combed hospital records from 2002 to 2007 and found 142 patients with surgically and pathologically proven acute cholecystitis. Of these, 75 (60 women and 15 men; mean age 68 years) had undergone a presurgical CT exam.
Two radiologists without knowledge of CT findings reviewed the images and examined the patients' medical charts for age, sex, clinical signs and symptoms, lab data, and clinical outcomes, comparing the findings for patients with and without gallbladder rupture.
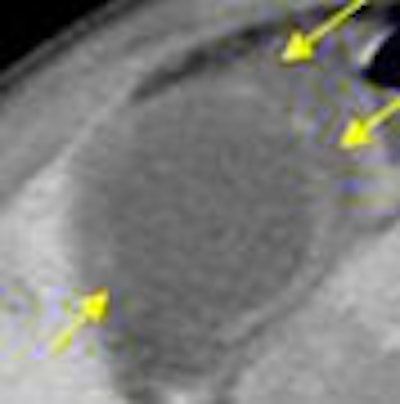
"Gallbladder rupture was seen in 16 of the 75, or about 21% of the cases," Chen said. "The most common CT findings included pericholecystic fat stranding in 71 of 75 patients, gallbladder wall enhancement, gallbladder wall thickening, and pericholecystic fluid collection."
In the analysis of CT images, "only seven findings showed significant differences between the rupture and the nonrupture group," he said. These included gallbladder wall defect (p = 0.000), intramural gas from the gallbladder (p = 0.043), intraluminal membrane of the gallbladder (p = 0.043), intraluminal gas of the gallbladder (p = 0.001), pericholecystic biloma or abscess (p = 0.009), free air (p = 0.001), and ascites (p = 0.019).

Perhaps most important, "the rupture group had a significantly higher mortality rate (18.8%) -- about 10 times that of the group without rupture" (1.7%), Chen said.
Multivariate analysis with logistic regression showed a significant association with gallbladder rupture in two findings: gallbladder wall defect (p = 0.0003, odds ratio: 30.18) and ascites (p = 0.049, odds ratio: 4.303).

As for limitations, the study was retrospective and was performed in patients with a high index of suspicion for acute cholecystitis and gallbladder rupture, Chen said.
"CT can effectively diagnose acute cholecystitis, with or without the complication of gallbladder rupture, and is recommended in the initial evaluation for clinical management decisions," he said.
By Eric Barnes
AuntMinnie.com staff writer
April 23, 2008
Related Reading
Lack of IV contrast causes discrepancy in CT with PET scans, November 22, 2007
MDCT's 'virtual Whipple' offers practice run before complex surgery, August 16, 2007
High contrast flow rate best for pancreas CT, November 8, 2006
Aw shucks! Corn-oil-based scintigraphy makes good in gallbladder disorder, January 20, 2005
Copyright © 2008 AuntMinnie.com