Physicians in Singapore are evaluating stent patency using extremely low radiation doses with the aid of dual-source MDCT, according to a presentation at the recent Society of Cardiovascular Computed Tomography (SCCT) meeting in Denver.
Nearly all studies were diagnostic, the group found, and the average radiation dose was less than 1 mSv.
"Dose considerations are an important part of our general approach to imaging patients these days," said consultant cardiologist Dr. Ho Kheng Thye, from Mount Alvernia Hospital in Singapore, in an interview with AuntMinnie.com.
Stent patency is more often examined now with coronary CT angiography than with invasive angiography, he said. The fact that there are so many indications for stent assessment (chest pain, dyspnea, postintervention, preoperative risk assessment, electrocardiogram abnormality assessment, and more) makes dose reduction a priority.
 |
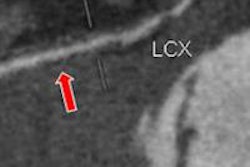
| Coronary CT angiography was performed in high-pitch flash mode after administration of atenolol and glyceryl trinitrate. The heart rate was 57 bpm, and the patient tolerated the procedure well at 100 kV with a total radiation dose of 0.85 mSv. Image courtesy of Dr. Ho Kheng Thye. |
The group from Alvernia Hospital and Tan Tok Seng Hospital in Singapore examined 50 patients (mean age, 55 ± 15 years; 66% male) with coronary stents from an initial cohort of 500 consecutive patients referred for coronary CT angiography over the course of a year.
All patients were scanned in flash mode on a dual-source CT scanner (Somatom Flash, Siemens Healthcare). The mean patient body mass index (BMI) was just 25.3 ± 3.9, and the tube current voltage was based on body weight:
- Less than 60 kg: 80 kV
- 60 to 100 kg: 100 kV
- More than 100 kg: 120 kV
The mean heart rate was 53 beats per minute (bpm) thanks to "aggressive" beta-blocking, he said. Of the group, 18% (n = 9) were scanned at 80 kV, 58% (n = 29) at 100 kV, and 24% (n = 12) at 120 kV following administration of 60 mL contrast and 60 mL saline at 5 mL per second.
Image quality was rated subjectively on a four-point scale depending on the degree of blurring -- with 1 being excellent and 4 nondiagnostic. The stents ranged in diameter from 2.75 to 4.0 mm.
Patients scanned at 80, 100, and 120 kV received doses of 0.38 ± 0.03 mSv, 0.90 ± 0.36 mSv, and 1.78 ± 0.15 mSv, respectively. One patient did not respond to beta-blockage (heart rate, 75 bpm) and was scanned in axial mode receiving a total dose of 2.46 mSv. The remaining 49 patients were scanned in flash mode.
In 95% of scans, the stented segments were of diagnostic quality (grades 1, 2, and 3).
"Generally those who didn't have calcium and had larger stent sizes were fine," he said. We had more problems with stents that were smaller than 3 mm, or if there was a combination of calcium and small stent size."
Ninety-nine percent of patients were eligible for imaging with the flash scan mode, which yielded consistent diagnostic quality imaging of coronary stents at a dose of less than 1 mSv, the authors concluded.
"High-pitch mode is good enough for general use," he said. "It's effective, but it is dependent on having a low and regular heart rate. If you control for the various parameters including heart rate, the experience is really good -- at least in our lab."