Persuaded by an analysis of clinical studies demonstrating the benefits of lung cancer screening, the American Cancer Society (ACS) on Friday published guidelines recommending CT screening for long-term current and former smokers. The new rules, however, hew closely to previous guidance that has been criticized as being overly cautious.
The ACS guidelines were nevertheless welcomed by screening advocates as another step on the road to routine CT lung cancer screening of current and former smokers.
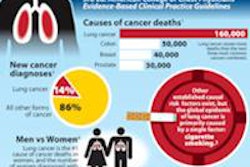
In preparing the recommendations, ACS joined with the American College of Chest Physicians (ACCP), the American Society of Clinical Oncology (ASCO), and the National Comprehensive Cancer Network (NCCN) to systematically review the evidence related to lung cancer screening with low-dose CT (LDCT). Based on the results of the National Lung Screening Trial (NLST) and a few other randomized, controlled trials, the researchers concluded that CT screening is warranted in individuals ages 55 to 74 years with at least 30 pack-years of smoking history, who are current smokers or who quit smoking within the past 15 years (CA: A Cancer Journal for Clinicians, January 11, 2013).
"Now that there is rigorous evidence supporting the value of screening for lung cancer with LDCT, it is important that the implementation of lung cancer screening proceeds in a manner that is focused on maximizing benefits and minimizing harms," wrote Dr. Richard Wender, chair of family and community medicine at Thomas Jefferson University Medical College, along with colleagues from more than a dozen other U.S. academic centers. "At this time, there is sufficient evidence to support screening provided that the patient has undergone a thorough discussion of the benefits, limitations, and risks, and can be screened in a setting with experience in lung cancer screening."
The careful recommendations were largely in line with the ASCO/ACCP guidelines by Bach et al published last May, which limit the number of individuals for whom screening is recommended. Screening under the new ACS guidelines, for example, requires a long smoking history and excludes other conditions that screening advocates have considered potentially appropriate indications, such as a history of chronic obstructive pulmonary disease (COPD), which is associated with an increased prevalence of lung cancer.
"It's a soft recommendation toward screening in a high-risk population," said Dr. Ella Kazerooni, professor of radiology at the University of Michigan, in an interview with AuntMinnie.com. "It's not a definite recommendation that the NLST-type people should go out and get screened; it's more like a recommendation that's trying to balance waiting for the NLST cost-effectiveness analysis to come forward, yet trying to do something to help those who may potentially benefit from screening to go out and learn more so that they may potentially want to get screened."
Benefits and harms
The ACS analysis focused on the potential benefits and harms of screening using low-dose CT, the identification of the groups of individuals likely to benefit or not benefit from a screening regimen, and the settings in which screening is likely to be effective, as well as recommendations about the screening process and the importance of smoking cessation.
For the primary end points of lung cancer mortality and all-cause mortality, only randomized, controlled trial data were considered. Observational data were included for other end points, particularly those related to screening performance in terms of false-positive results, frequency of additional tests indicated, and smoking cessation rates, for a total of eight randomized trials and 13 cohort studies.
At the same time, the authors of the guidelines suggested, as Bach et al before them did, that the 20% mortality reduction shown in NLST was only a minimum and should be explored further. And in the new guidelines, the authors stated that three annual screening rounds may not be sufficient to garner the maximum benefit from CT screening.
"There is some uncertainty as to whether a 20% difference in lung cancer deaths is the ultimate mortality reduction that can be expected from LDCT screening," Wender and colleagues wrote. "First, there were only three [low-dose] CT examinations given in the NLST. ... Second, there actually may have been some, albeit small, benefit from [chest x-ray] that contributed to a smaller difference in the lung cancer death rates between the two arms than would have been observed if the patients in the comparison arm had just received usual care."
They added that in more than one study, the detection of stage I cancers doubled when chest x-ray was included versus usual care alone, suggesting a small, if hidden, benefit to chest x-ray.
The authors also noted that nearly 40% of CT screening subjects in NLST had an abnormal result somewhere in the first three scans, though false-positive findings tended to start higher and diminish with later rounds of screening.
"Prior to resolution, false-positive findings can cause anxiety and lead to additional costs, additional radiation exposures, and invasive procedures," the authors wrote. "One study reported that indeterminate lung cancer screening test results increased anxiety, but that anxiety diminished over time, a finding similar to what has been observed in breast cancer screening."
Recommendations
The authors recommended that clinicians ascertain the smoking status and history of patients ages 55 to 74 years.
"Clinicians with access to high-volume, high-quality lung cancer screening and treatment centers should initiate a discussion about lung cancer screening with patients aged 55 years to 74 years who have at least a 30 pack-year smoking history, currently smoke, or have quit within the past 15 years, and who are in relatively good health," they wrote.
Clinicians should discuss the limitations of CT with potential screening subjects and emphasize that it will not detect all lung cancers or prevent all deaths, in addition to discussing the potential harms from invasive procedures, they wrote. Finally, Wender and colleagues emphasized the importance of smoking cessation counseling with potential screening subjects.
"Eligible patients should make the screening decision together with their healthcare provider," they wrote. "Helping individuals to clarify their personal values can facilitate effective decision-making."
Healthcare providers should not discuss screening with patients who do not fall into the appropriate risk category to recommend screening, they added.
As for the risk of overdiagnosis from screening, the authors noted that there was only a 13% difference in the number of cases diagnosed in the CT versus the chest x-ray arm of the study, and that it was too early to draw any conclusions about overdiagnosis in lung cancer screening with CT.
Importantly, a subgroup analysis of the NLST results to determine whether screening benefits varied by smoking history is not yet available, and whether the benefits exceed the harms in any subgroup or hit the mark in terms of cost-effectiveness "are questions that cannot be answered at this time," they wrote. In any case, the authors recommend that screening occur in high-volume centers where expert screening is available.
Commentary from lung cancer screening experts
"I thought it was a wonderful review of the literature that really summarized all the pertinent information that we know about lung cancer screening with CT to date ... but it really didn't add substantively to the discussion, and I don't think it will change the landscape of what's currently going on in lung cancer screening," said Kazerooni. "I think people were looking for a stronger recommendation."
The NLST's cost-effectiveness analysis, which is expected to be available in the next three to six months, could go a long way toward adding certainty to screening recommendations from all sides, she said. For now, many screening advocates are leaning more toward the recommendations of the NCCN, an alliance of 21 leading cancer centers worldwide. In addition to the strict NLST criteria, NCCN has suggested a possible benefit of screening for patients who are younger than 55, or perhaps have fewer than 30 pack-years of smoking history.
Dr. David Yankelevitz, professor of radiology at Mount Sinai Medical Center, said he also leans toward more liberal screening guidelines.
"I personally think it should be expanded" to include screening for wider groups of individuals at risk, he said. But he emphasized that the ACS authors made important progress toward broader screening criteria in several areas.
The ACS authors "do a lot of things that are interesting and positive and different from some of the other guidelines," Yankelevitz told AuntMinnie.com. "For example, they endorse annual screening up until [age] 74 -- they don't say stop after three rounds like some of these other guidelines. That's a big statement. They're recognizing that you shouldn't think of [screening] in terms of a single round ... but rather in terms of having a benefit in each annual round and that that benefit persists beyond the three rounds."
In the ACS discussion of overdiagnosis, where the prevailing opinion for years has been that the extent of overdiagnosis is likely to be significant with CT, "here, the discussion concludes that it's probably going to be insignificant," allowing that overdiagnosis is a possibility but likely doesn't represent a significant fraction of cases, he said. "That's a very powerful statement from ACS."
For its part, the American College of Radiology (ACR) cautioned that regardless of the recommendations coming out in various papers, the pieces aren't yet in place for widespread screening.
"What we want people to know, if they are to see these recommendations and say [screening] needs to be done right this second, [is] that the infrastructure is not in place yet for a widespread national screening program," ACR spokesperson Shawn Farley told AuntMinnie.com. "That infrastructure needs to be in place to ensure a uniform, quality baseline of this type of care nationwide, so that the person who wants to be screened in a more rural part of the country can expect the same type of lifesaving benefit from these exams as a patient who goes into a large medical center in a large metropolitan area. And that's going to take some time."
Laurie Fenton-Ambrose, president and CEO of the screening advocacy group Lung Cancer Alliance, said it's encouraging to see yet another organization produce guidelines affirming the benefits of lung cancer screening, whether or not they might be considered more restrictive than other recommendations.
"From our perspective, the most important issue is putting this into practice responsibly," she said. "We are working, as we have been for the past year, on our National Framework of Excellence for lung cancer screening, which is establishing the rights of consumers, the right to know they are at risk, and the right to know where to go for responsible care."
As for who, precisely, should be screened, "the challenge is that people are looking at the NLST as if they're frozen in that moment of time," she said. "Since that trial was halted, both the technology and the workups for how we screen and who is at risk have [evolved] to a much deeper and greater understanding."
"So we're going to continue to work with medical centers and professional societies that are embracing the NCCN recommendations, and follow those best practices, but most importantly make sure consumers have information that will allow them to determine if they should be screened, and to do it at a place that's experienced," she said.
The recommendations will broaden with time, she added. "I think that most experts in this field clearly recognize that there are others who fall within a high-risk category beyond what the NLST provided."