Model-based iterative reconstruction (MBIR) can help identify vulnerable plaque at CT, potentially improving prediction for a particularly dangerous source of cardiovascular events, according to a study presented at RSNA 2013.
Researchers from Massachusetts General Hospital (MGH) looked at vulnerable plaque and found an association between plaque areas less than 60 HU at CT and the presence of lipid core plaque at histology, regardless of the reconstruction scheme.
When it came to identifying the dangerous plaques, however, they found that use of model-based iterative reconstruction (GE Healthcare) conferred a significant advantage in sensitivity over the earlier-generation advanced statistical iterative reconstruction (ASIR, GE), as well as filtered back projection (FBP).
The study showed that MBIR can improve radiologists' ability to detect vulnerable plaque at coronary CT angiography (CCTA), said Dr. Stefan Puchner in his RSNA presentation.
"The identification of vulnerable plaque is obviously very important as we know it leads to thrombosis," he said. The plaque's telltale large lipid core and thick fibrous cap have been shown to correlate with findings at intravascular ultrasound, but the jury is still out on whether CT findings correspond with histology.
"If CCTA can, indeed, detect these vulnerable features, vulnerable plaque assessment could be improved given good image quality," Puchner said. "So the aims of this study were to evaluate the accuracy of three algorithms [MBIR, ASIR, and FBP] for the detection of lipid core plaque."
Puchner and colleagues, including Dr. Maros Ferencik, PhD; Dr. Pal Maurovich-Horvat, PhD; and Dr. Udo Hoffmann, obtained CT and histological data from the coronary arteries of three ex-vivo hearts, reconstructing the images using FBP, ASIR, and MBIR, Puchner said.
After scanning, the group coregistered all of the cross-sectional images between the three reconstruction algorithms. Next, they coregistered all of the resulting CCTA "triplets" with histological data.
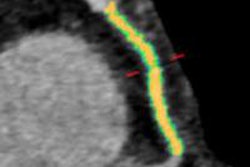
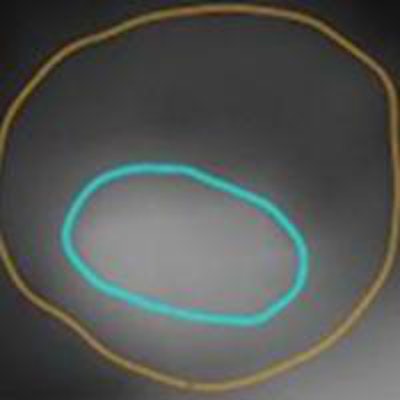
 Coregistered filtered back projection reconstruction (FBPR)/ASIR/MBIR "triplet" with histology. Images courtesy of Dr. Stefan Puchner.
Coregistered filtered back projection reconstruction (FBPR)/ASIR/MBIR "triplet" with histology. Images courtesy of Dr. Stefan Puchner.The researchers compared the median (interquartile range) between reconstruction methods using the Wilcoxon rank sum test, and they also used area under the curve (AUC) to measure diagnostic accuracy using logistic regression analysis.
Plaque areas visualized at less than 60 HU, corresponding to the lipid core, were assessed semiautomatically with software to define regions of lipid/necrotic core 200 mm and larger with a circumference greater than 60°, and a fibrous cap thickness larger than 450 mm at histology. Automatic software assessment of 0.5-mm cross-sections was supplemented with manual correction of the contours in each reconstruction method when needed.
"In total, the cross-sections that needed manual correction were 37% for FBP, 36% for ASIR, and 27% for MBIR, so iterative reconstruction algorithms allowed for fewer corrections," Puchner noted.
The total study sample included 173 FBP/ASIR/MBIR "triplets" corresponding to histologic cross-sections from the three hearts.
"Looking at sensitivity and specificity, we see that MBIR retains high sensitivity and specificity of 90%, while other reconstruction algorithms show a decrease in sensitivity and an increase in specificity," he said.
| FBP/MBIR/ASIR for detection of lipid core plaque per histology | ||
| Reconstruction algorithm | Cutoff for plaque area < 60 HU at CCTA (mm2) | Sensitivity |
| Predefined specificity of 70% | ||
| FBP | 4.01 | 92% |
| ASIR | 3.80 | 92% |
| MBIR | 4.17 | 92% |
| Predefined specificity of 80% | ||
| FBP | 4.84 | 65% |
| ASIR | 5.04 | 69% |
| MBIR | 4.90 | 81% |
| Predefined specificity of 90% | ||
| FBP | 5.96 | 42% |
| ASIR | 5.93 | 46% |
| MBIR | 5.91 | 69% |
Regarding plaque characteristics in general, for plaque areas less than 60 HU, all reconstruction methods yielded significantly larger lipid core plaque sizes compared with nonlipid core plaque, with MBIR as the largest (5.17 mm2 versus 3.16 mm2 for FBP, 5.58 mm2 versus 3.17 mm2 for ASIR, and 6.50 mm2 versus 3.23 mm2 for MBIR; all p < 0.0001).
This produced an AUC for detecting lipid core plaque of 0.803 for FBP, 0.850 for ASIR, and 0.903 for MBIR, Puchner said.
"On the other hand, for plaque above 180 HU, this area was smaller in MBIR than in the other reconstruction algorithms," he said. Overall, "the area of plaque defined by CCTA was generally higher in sections with lipid core plaque and lower in cross-sections with no lipid core, regardless of the reconstruction algorithm."
"Plaque area below 60 HU in CCTA was associated with the presence of lipid core plaque as determined by histology, irrespective of reconstruction algorithm," Puchner concluded. "MBIR showed significantly higher diagnostic accuracy for detection of lipid core plaque compared to ASIR and filtered back projection."
Model-based iterative reconstruction enhances the accuracy of CCTA for detecting and characterizing vulnerable plaque noninvasively, the researchers concluded.