Nearly half of all patients who test positive on SPECT myocardial perfusion imaging (MPI) are found to be negative at coronary CT angiography (CCTA), according to a study by researchers from the U.S. and Germany. The findings call into question the routine use of SPECT MPI, a test that has been a mainstay of the diagnostic workup of patients with a clinical suspicion of coronary artery disease (CAD).
Not only were many of SPECT's ischemia results mostly unconfirmed at CCTA, but the latter test showed perfect sensitivity and 84% specificity compared with invasive coronary angiography, which was used as a reference standard test, according to the results of the study by researchers from Ludwig Maximilian University of Munich and the Medical University of South Carolina in Charleston.
"Almost half of patients who are shown to have clinically suspected coronary artery disease and have an abnormal nuclear perfusion study demonstrate no potentially obstructive disease at coronary CT angiography," said Dr. Felix Meinel in a presentation at ECR 2015 in Vienna.
A widely used test
At least in the U.S., myocardial perfusion imaging is a widely used imaging test for suspected coronary artery disease patients who have an abnormal test results at nuclear perfusion imaging, said Meinel, who is from Ludwig Maximilian University of Munich.
 Dr. Felix Meinel from Ludwig Maximilian University of Munich and the Medical University of South Carolina.
Dr. Felix Meinel from Ludwig Maximilian University of Munich and the Medical University of South Carolina.Such patients "are then typically directly referred to the cath lab for invasive angiography; however, we know that many of these patients will not show obstructive lesions at invasive angiography," Meinel said. "So the question arises: Is there potentially a role for coronary CTA in this relatively high-risk cohort of patients who already have abnormal nuclear perfusion studies?"
The study aimed to determine the diagnostic yield of coronary artery disease in patients who are clinically referred for invasive coronary angiography based on a clinical concern for CAD and a recent abnormal stress nuclear perfusion study, Meinel said. The study team prospectively scanned 100 patients (84 men, 16 women; mean age 59.6 ± 8.9 years) suspected of having CAD, excluding patients with prior revascularizations or contraindications to any of the tests.
The nuclear tests were performed using a standard stress-rest SPECT protocol with either treadmill (n = 61) or pharmacological (n = 39) stress, Meinel said. Perfusion abnormalities were classified as reversible, fixed, or mixed with transient ischemic dilatation or other abnormalities. After injection of 60 mL to 120 mL of iodinated contrast, CCTA was performed according to standard guidelines using beta-blockers and sublingual nitroglycerin, with electrocardiogram gating or prospective triggering depending on the patient's heart rate and rhythm.
Over the course of the study, the institution transitioned from a 64-detector-row scanner used in 2008-2009 to a dual-source CT used in 2010-2013 (both Siemens Healthcare). The researchers rated coronary vessels as having no luminal narrowing, nonobstructive disease, or potentially obstructive disease, which was defined as 50% stenosis or greater for the study.
Invasive angiography served as the reference standard and was counted as positive for clinically significant disease if there was at least one 50% or greater stenosis in the left main artery or 70% or greater stenosis in any other major coronary segment, corresponding to the levels used to recommend revascularization.
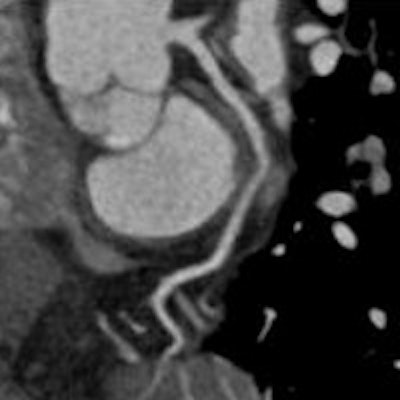
 Above, patient whose SPECT exam was read as positive for inferior wall ischemia. However, neither CCTA nor catheter angiography showed evidence of coronary artery disease. Images courtesy of Dr. Felix Meinel.
Above, patient whose SPECT exam was read as positive for inferior wall ischemia. However, neither CCTA nor catheter angiography showed evidence of coronary artery disease. Images courtesy of Dr. Felix Meinel.Half as much significant disease at CCTA
At CCTA, 54% of patients had at least one 50% or greater stenosis, while 92% had perfusion abnormalities at SPECT MPI, the authors reported.
At SPECT MPI, most of the perfusion abnormalities were reversible perfusion defects and ischemia, according to Meinel. The fact that only 54% of patients had stenosis indicates "that almost half of patients did not have a potentially obstructive lesion ... and almost one-third of patients had no luminal narrowing at all," he said.
| SPECT MPI findings | |
| Abnormality | No. of patients |
| Perfusion abnormalities | 96 |
| Reversible perfusion defect (ischemia) | 82 |
| Fixed perfusion defect (infarction) | 2 |
| Mixed (partly reversible perfusion defect) | 12 |
| Transient ischemic dilatation | 18 |
| Reduced ejection fraction | 26 |
| Other | 2 |
| CCTA findings | |
| Finding | No. of patients |
| Potentially obstructive CAD (≥ 50% stenosis) | 54 |
| Single-vessel disease | 23 |
| Two-vessel disease | 14 |
| Three-vessel disease | 17 |
| Location of potentially obstructive CAD | |
| Left anterior descending (including left main) | 42 |
| Left circumflex artery | 31 |
| Right coronary artery | 29 |
| Nonobstructive disease (1% to 49% stenosis) | 14 |
| No luminal narrowing (0% stenosis) | 32 |
Comparing CCTA with invasive angiography yielded sensitivity of 100% and specificity of 84% for clinically significant CAD, Meinel noted. On a per-patient basis, CCTA delivered a 100% negative predictive value and 83% positive predictive value for clinically significant coronary disease.
The study had limitations, in that the reference standard in the study was visual assessment of invasive angiography by cardiologists, which is not the perfect reference standard, Meinel said. The population was predominantly male and Caucasian, so gender or ethnic bias cannot be ruled out, he added.
Still, the data make two things clear, he said. First, almost half of patients who are shown to have clinically suspected coronary artery disease and have an abnormal nuclear perfusion study demonstrate no potentially obstructive lesions at CCTA.
Second, he said, "Coronary CTA, even in this relatively high-risk group of patients, has high sensitivity and a high negative predictive value, and can thus be considered as the next diagnostic step after an abnormal nuclear perfusion study."
An audience member Dr. Rozemarijn Vliegenthart, from the University Medical Center Groningen in the Netherlands, asked if SPECT with its 50% false-positive rate should still be used routinely in these patients, or should CT be used as the initial test.
"We're not necessarily saying that the SPECT was all false-positive," Meinel responded. "We're just saying there are differences between anatomic and functional testing, and the two tests don't always correlate very well. These patients might have microvascular disease. All we're saying is that with CT we can exclude macroscopic anatomical disease that would be potentially treatable with a cathether."
The SPECT positives "might have ischemia but they don't have lesions that would need a catheter," Meinel said. Probably very few actually have microvascular disease, he added.


















