A novel CT angiography (CTA) technique using nongated high-pitch images and iterative reconstruction delivered diagnostic scans across the board at about one-tenth the dose of standard exams, along with fewer motion artifacts and lower contrast media requirements, concludes a new study in Academic Radiology.
On the negative side, the study of 67 Chinese patients revealed higher mean noise values in the high-pitch group versus the standard-pitch scans, along with lower signal-to-noise (S/N) and contrast-to-noise (C/N) ratios, the study team wrote. However, the studies were diagnostic and image quality was high.
"It is important to note that this [ultralow-dose] protocol did not compromise diagnostic information, as both readers rated all CTA examinations as diagnostic," wrote lead author Dr. Long Jiang Zhang, PhD, and colleagues from Nanjing University Medical School in Nanjing, China, and the Medical University of South Carolina (MUSC) in Charleston (Acad Radiol, April 11, 2015).
Radiation dose can add up
CTA has become the gold standard for assessing the aorta, as well as the preferred modality for follow-up exams in patients with thoracic aortic disease. However, long-range scanning coverage of the aorta over many follow-up exams leads to a high cumulative radiation dose.
"Thus, reducing the radiation dose of aortic CTA is of great interest," Zhang and colleagues wrote.
Previous studies have looked at radiation dose reduction using a variety of techniques, including lower tube voltage, automatic tube voltage selection, and high pitch or iterative reconstruction. But no study has combined them all to optimize the techniques in combination, in particular CTA scanning at 70 kVp, which has recently shown promise.
"It is known that lower tube voltages allow the reduction of contrast agent as the attenuation of iodinated contrast agent increases at low tube voltages," the authors wrote.
Therefore, the authors sought to assess the feasibility of high-pitch 70-kVp CTA of the thoracic aorta with 40 mL of contrast, and compare it with standard-pitch CTA at 100 kVp with 60 mL of contrast.
In group A, 31 patients with a mean age of 55 ± 14 years underwent aortic CTA at 70 kVp (pitch, 3.4; 40-mL contrast dose). Meanwhile, 36 patients in group B underwent CTA at 100 kVp (pitch, 1.2; 60-mL contrast dose).
All CTA exams were performed on a second-generation dual-source CT scanner (Somatom Definition Flash, Siemens Healthcare) at 64 x 2 x 0.6-mm collimation, 280-msec gantry rotation, and an effective tube current-time product of 320 mAs per rotation. All exams were performed without electrocardiogram (ECG) gating to reduce the radiation dose as much as possible.
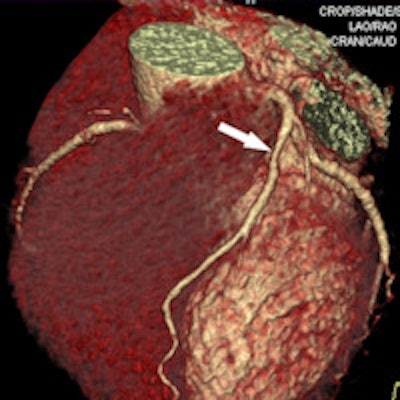
 66-year-old male with suspected coronary artery disease. 50% stenosis in the left anterior descending (LAD) artery is seen at CTA (above) and digital subtraction angiography (below). Images courtesy of Dr. Long Jiang Zhang, PhD.
66-year-old male with suspected coronary artery disease. 50% stenosis in the left anterior descending (LAD) artery is seen at CTA (above) and digital subtraction angiography (below). Images courtesy of Dr. Long Jiang Zhang, PhD.Because the aorta is larger than the coronary arteries, gated exams are unnecessary, noted study co-author Dr. U. Joseph Schoepf from MUSC, who discussed the study in an interview with AuntMinnie.com.
"But at a busy center such as in China, it probably makes sense not to because it takes time to put ECG leads on the patient," he said. "The clinicians may dispense with gating to no negative effect to speed workflow in China's very high throughput centers."
At MUSC, synchronization is included in 78-mAs exams.
"In that high-pitch mode, you can actually do that without any penalty in scan duration or radiation dose, so the scan doesn't take any longer or use any more radiation," Schoepf said. "Obese patients don't matter much."
The authors evaluated vascular enhancement quantitatively by measuring attenuation in the aorta at different levels. Image quality was independently evaluated by two experienced readers who were blinded to the acquisition protocol.
To assess dose output, the authors recorded CT dose index volume (CTDIvol) and dose-length product (DLP) for each scan. Effective dose was estimated by multiplying DLP by the standard conversion factor.
In group A, four patients had aortic aneurysms, 10 had arteriosclerosis, and 13 had follow-up examinations after endovascular treatment of aortic dissection. Aortic disease was excluded in five patients.
As for group B, the researchers reported aneurysmal aortic disease in three patients, atherosclerosis in 15 patients, endovascular devices in cases of aortic dissection in 10 patients, aortic dissection in one patient, and negative results in seven patients. No significant age or gender differences were seen between the groups.
Fast scans noisier, but less motion artifact
In group A, CT attenuation and image noise levels of all evaluated areas were higher than those in group B (p < 0.001), while S/N and C/N ratios in group A were lower than in group B (p < 0.001), the team reported.
On a scale of 1 to 3, with 1 representing excellent image quality, the quality of the diaphragmatic aorta was inferior in group A, with a rating of 1.26, compared with 1.06 for group B (p < 0.05). But no differences were seen between the groups in image quality at the aortic arch, with a rating of 1.06 for group A and 1.03 for group B, nor in the pulmonary trunk (p > 0.05 for both).
However, owing to faster scan times, the researchers found markedly decreased motion artifact in the high-pitch group A versus standard-pitch group B, which resulted in increased image quality levels at this location.
"Both readers believed both CTA protocols sufficiently addressed the diagnostic task at hand," the authors wrote.
Drastically reduced dose
Radiation dose as measured by mean entrance dose was 0.4 mSv for thoracic aortic CT imaging at 70 kVp, representing an 85% reduction versus 2.7 mSv with the 100-kVp acquisition mode, the group reported. Prior studies showed that entrance dose could be as high as 26 mSv for aortic CTA with retrospective ECG gating. Compared with group B, CTDIvol of group A was reduced by 85.7% and DLP was reduced by 83.6%.
The results are to be expected due to the ultralow tube voltage used in the study, and because the attenuation coefficient of iodine "increases when photon energy decreases toward the k edge," the group wrote.
Limitations of the study include its small sample size. In addition, the 70-kV setting as well as the 40-mL contrast dose was fixed without regard to clinical applications, according to the authors. Also, the results in a second-generation dual-source CT scanner may be limited for obese patients owing to increases in image noise; this limitation might be resolved with a third-generation dual-source scanner that has a peak tube current of up to 1,300 mAs.
As for future investigations, "I don't really think we need more research to look into the image quality or accuracy," Schoepf said. "I think we should be more concerned about what this does to patient safety."
For example, maybe the incidence of volume overload will decrease with this reduced contrast approach, Schoepf said. With contrast injection, having too much volume in the circulatory system can lead to problems such as pulmonary edema "because the heart cannot put up with the increased volume that it has to pump all of the sudden."
Along these lines, future research will be helpful for "pushing the envelope" to further reduce contrast media use, perhaps down to as low as 30 mL when imaging is limited to the thoracic aorta, he said.

















