Nearly one-third fewer patients presenting to the emergency department with blunt abdominopelvic trauma ended up getting a CT scan after a Boston hospital implemented a clinical algorithm to triage patients away from unnecessary CT exams, according to a new study published September 12 in Radiology.
Researchers from Boston University Medical Center compared CT use in more than 13,000 patients who were treated with or without use of the algorithm, which is intended to eliminate unnecessary CT scans. Not only did CT use decline by 30% with use of the algorithm, but the percentage of positive scans increased, and the average length of hospital stays decreased without a corresponding increase in mortality (Radiology, September 12, 2016).
"The main thing to me was the drop in the number of CT studies and with no serious missed abnormalities," said lead author Dr. Arthur Baghdanian in an interview with AuntMinnie.com.
Benefits lead to overuse
Most trauma patients present to the emergency department with blunt injuries, most commonly due to motor vehicle collisions. Minimizing the time to diagnosis is key to reducing mortality and morbidity and cutting hospital stays. CT is a quick way to identify important injuries and discharge those with negative results, and its use has helped to reduce laparotomy rates and the need for invasive angiography.
 Dr. Arthur Baghdanian from Boston University Medical Center.
Dr. Arthur Baghdanian from Boston University Medical Center.Unfortunately, CT's benefits have led to continued overuse in the emergency department, despite continued moderation of CT use in other settings. Negative effects of CT overuse include increased costs, unnecessary radiation exposure, and inefficient use of resources, the authors wrote.
"In 2010 the interdisciplinary committee, the trauma surgeon team, and radiology continued to see an increase in CT use -- 83% of the patients who walked in the door would get a CT scan," Baghdanian said.
That's when the group set out to create a series of triage algorithms to separate various categories of trauma patients needing scans from those who were expected to do OK without a scan, he said.
Based on an existing trauma registry, the retrospective study included 13,096 adult patients (mean age, 42 years) admitted with blunt abdominopelvic trauma during an eight-year period. Patients were divided into two groups: those admitted between January 2006 and June 2010, known as the prealgorithm group, and those admitted between July 2010 and December 2014, known as the postalgorithm group.
Data collected for the study included the number of CT exams at admission, positive blunt abdominopelvic trauma findings, injury severity score, length of hospital stay, and mortalities.
Clinical exam findings favoring CT
The diagnostic algorithm begins in the clinical exam, sorting for signs of serious injury based on the literature and the hospital's existing trauma registry, and referring patients with signs of injury to CT. Patients also get portable radiography exams.
First, the patient has to be conscious for triage because the clinician is looking for an accurate assessment of pain, Baghdanian said. Patients are assessed for signs of a high-speed injury such as fracture of the first two ribs, as well as vascular injury such as hypertension or instability fractures of the pelvic ring.
Patients who are unstable will likely go straight to laparotomy, but if blood pressure is normal and the patient can participate in the evaluation, a CT scan showing no intra-abdominal injury can avoid intervention, Baghdanian said.
When patients can participate in a medical history discussion, the clinician can look for signs of bruising or abrasion along the abdominal wall, or a lap-belt injury that could results in mesenteric tears, all indicating the need for CT.
The clinician looks for gross hematuria and abdominal tenderness, fractures, and evidence of spinal cord injury for a CT referral.
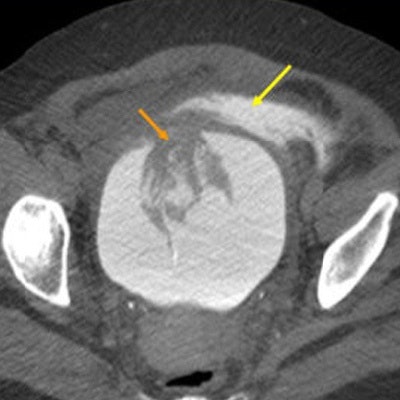
 Simple extraperitoneal rupture seen in a CT scan of a 55-year-old man who fell down five concrete steps. Gross hematuria in the Foley catheter was noted. CT cystogram demonstrates a large anterior bladder wall defect (orange arrow) with contrast seen pooling in the pelvic extraperitoneal space (yellow arrow). The patient was taken to the operating room and found to have an 8-cm longitudinal bladder perforation. Images courtesy of Dr. Arthur Baghdanian.
Simple extraperitoneal rupture seen in a CT scan of a 55-year-old man who fell down five concrete steps. Gross hematuria in the Foley catheter was noted. CT cystogram demonstrates a large anterior bladder wall defect (orange arrow) with contrast seen pooling in the pelvic extraperitoneal space (yellow arrow). The patient was taken to the operating room and found to have an 8-cm longitudinal bladder perforation. Images courtesy of Dr. Arthur Baghdanian.Absent important clinical findings or in the presence of certain comorbidities, patients can skip CT and be admitted for observation for 24 hours, or they can be discharged, depending on the findings and history, Baghdanian said. Patients on blood thinners, those undergoing hemodialysis, and those with cirrhosis, blood platelet counts less than 50,000, or New York Heart Association classification scores of 3 or 4 are admitted for observation or discharged without CT.
Indications for CT are as follows:
- Visceral injury, including the liver, bowel, kidney, bladder, pancreas, spleen, and adrenal glands
- Vascular injury, including aneurysm, pseudoaneurysm, laceration, hematoma, and active extravasation of any major vessel
- Intraperitoneal simple fluid, including dense intraperitoneal fluid, retroperitoneal fluid, and hematoma
- Miscellaneous findings of the mesentery and diaphragm, and anterior abdominal wall hematoma
CT scans of the abdomen and pelvis were acquired on a 64-detector-row scanner (LightSpeed VCT, GE Healthcare) using a reconstruction thickness of 1.35 and 3.75 mm, pitch of 1, and gantry rotation time of 0.5 seconds. Images were obtained following intravenous administration of contrast media using a dual-syringe power injector (Stellant, Medrad).
Far fewer CT scans
Patients who were seen after the algorithm went into effect were significantly less likely to undergo a CT scan (44%, 2,413 of 5,408) than the prealgorithm patients (76.7%, 5,900 of 7,688), a decrease of 32.1%.
Meanwhile, the mean injury severity score of patients who had a CT scan rose from 10.1 to 13.3 after the algorithm, indicating that CT was being used to examine more seriously injured patients.
Also, the percentage of exams with trauma-related findings rose from 17.1% to 19.8% with the algorithm. Hospital stays and mortality both fell slightly.
| Findings before and after algorithm implementation | |||
| Parameter | Before algorithm | After algorithm | p-value |
| Patients admitted to emergency department who had CT | 76.7% | 44.6% | < 0.001 |
| Admission CT exams with positive findings | 17.1% | 19.8% | 0.003 |
| Admission CT exams with positive findings excluding free fluid | 12.3% | 17.5% | < 0.001 |
| Mean mortality | 3.1% | 2.7% | 0.19 |
| Mean No. of days in hospital | 4.8 | 4.2 | < 0.001 |
"The implementation of a clinical triaging algorithm for abdominopelvic trauma at our level I trauma center resulted in decreased use of CT examinations of the abdomen and pelvis," the authors wrote. Positive findings increased, the length of stay decreased, and mortality dropped slightly with use of the algorithm, but the difference was not significant.
The researchers found slightly higher complication and readmission rates in the non-CT group, but after reviewing 1,200 cases, "the conclusion was made that no case demonstrated missed trauma-related injuries that occurred as a result of the clinical triaging algorithm, which further supported the conclusion that no trauma-related injuries were missed by using this approach," Baghdanian and colleagues wrote.
Still, not including all of the patients in the review was a study limitation, they noted. Another limitation was the retrospective study design. Without a rereview of the CT images, findings missed originally could not be detected.
The study demonstrates that institutional clinical triaging algorithms can be implemented to prevent unnecessary CT examinations in patients with blunt abdominopelvic trauma in an ongoing effort to reduce unnecessary imaging, the group concluded.
A major advantage of having the algorithm in place is that the emergency room doctors don't have to go it alone, Baghdanian said.
"We're putting it on everyone as a team, where you now have surgery, radiology, and ER present, and you don't have to base the decision on your own experience or criteria," he said.
As for future work, follow-up should cover everyone rather than a sample of the patients, with more stringent criteria for readmissions, he said. In addition, a cost analysis will be needed. As for fully implementing the algorithm in clinical practice, the team is taking a go-slow approach, mindful of the potential of missing an injury.
Next up, the group is preparing to analyze a similar algorithm in place for head and neck trauma, Baghdanian said.


















