The presence of ground-glass opacities (GGO) rather than pure-solid nodules on CT lung cancer imaging is an encouraging prognostic factor in non-small cell lung cancer (NSCLC), researchers have reported.
A team led by Meiling Li, MD, of Shanghai Jiao Tong University School of Medicine in China, found that minor-GGO elements on lung CT (equal to or less than 10%) were associated with a decreased likelihood of recurrence. The results were published May 29 in the American Journal of Roentgenology.
"Among patients with clinical stage 1 NSCLC, cancers with a minor-GGO component were associated with a better prognosis versus those with a pure-solid appearance," the group noted.
The presence of GGO is a favorable prognostic factor in NSCLC, but what has been less understood is the impact of small GGO components on the prognosis of clinical stage 1 NSCLC in comparison with pure-solid nodules, Li's group explained.
To fill the knowledge gap, Li and colleagues conducted a study that included 382 patients who underwent surgical resection between January and December 2015 for stage 1 NSCLC that had been identified on preoperative chest CT as a nodule with a consolidation-to-tumor ratio between ≥ 0.9 and < 1.0. Two radiologists assigned the nodules to minor GGO or pure-solid categories; the investigators assessed recurrence-free survival and cancer-specific survival by Kaplan–Meier curves.
Both radiologists agreed on all nodule classifications. The team found the following:
- Compared with the pure-solid group, the minor-GGO group showed better five-year recurrence-free survival (83.4% vs. 55%; p < 0.001) and better five-year cancer-specific survival (92.4% vs. 76.4%, p = 0.004).
- A minor-GGO component was linked to decreased likelihood of disease recurrence (HR = 0.37, p = 0.001).
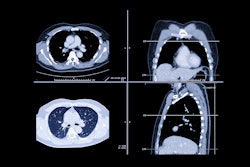
 62-year-old man without smoking history who presents with lung nodule. Axial contrast-enhanced CT images on lung windows (A) and mediastinal windows (B) show subsolid nodule in left upper lobe with total diameter of 2.4 cm (solid line) and diameter of solid component of 2.2 cm (dotted line). Consolidation to tumor was 0.92. Nodule was resected and diagnosed as acinar-predominant adenocarcinoma (acinar component 65%, papillary component 30%, micropapillary component 5%) with epidermal growth factor receptor mutation. Patient showed no evidence of recurrence or cancer-specific death after 81 months of follow-up. Image and caption courtesy of the American Roentgen Ray Society (ARRS).
62-year-old man without smoking history who presents with lung nodule. Axial contrast-enhanced CT images on lung windows (A) and mediastinal windows (B) show subsolid nodule in left upper lobe with total diameter of 2.4 cm (solid line) and diameter of solid component of 2.2 cm (dotted line). Consolidation to tumor was 0.92. Nodule was resected and diagnosed as acinar-predominant adenocarcinoma (acinar component 65%, papillary component 30%, micropapillary component 5%) with epidermal growth factor receptor mutation. Patient showed no evidence of recurrence or cancer-specific death after 81 months of follow-up. Image and caption courtesy of the American Roentgen Ray Society (ARRS).
"Among patients with clinical stage 1 NSCLC, cancers with a minor-GGO component were associated with a better prognosis versus those with a pure-solid appearance," the group concluded. "Radiologists encountering predominantly solid nodules on CT should carefully assess images for even a minor-GGO component given the favorable prognosis."
The complete study can be found here.