This article is the 11th in our series of white papers on radiologic patient positioning techniques for x-ray examinations. If you'd like to comment on or contribute to this series, please e-mail
Radiographic positioning of the forearm
Radiographic examination of the forearm is performed using anteroposterior (AP) and lateral projections. Both projections of the forearm demonstrate the elbow joint, the radius and the ulna, and the proximal row of slightly distorted carpal bones.
Technical factors
- Image receptor (IR): Lengthwise 11 x 14 inch (30 x 35 cm) divided; 7 x 17 inch (18 x 43 cm) single; 14 x 17 inch ( 35 x 43 cm) divided.
- Detail screen, tabletop.
- In a lateral projection, place the elbow at the cathode end of the x-ray beam to make best use of the anode-heel effect.
- 60 to 65 kVp range, mAs 6.
- Minimum SID of 100 cm.
Positioning for an AP projection of the forearm
- Seat the patient close to the radiographic table and low enough to place the entire limb in the same horizontal plane.
- Supinate the hand, extend the elbow, and center the unmasked half of the cassette to the forearm. Ensure that both the wrist and elbow joints are included.
- The long axis of the forearm should be aligned to the long axis of the IR
- Ask the patient to lean laterally until the forearm is in a true supinated position, and adjust the humeral epicondyles so they are equidistant from the cassette.
- Ensure that the hand is supinated. Pronation of the hand crosses the radius over the ulna at its proximal third and rotates the humerus medially, resulting in an oblique projection of the forearm.
- The central ray (CR) should be perpendicular to the midpoint of the forearm.
Evaluation criteria
- The entire radius and ulna should be visible, with pertinent soft tissues, such as fat pads and stripes of the wrist and elbow joints.
- The wrist (along with the proximal carpal row) and distal humerus should be clearly demonstrated.
- No rotation as evidenced by humeral epicondyles visualized in profile with slight superimposition of the radial head, neck, and tuberosity over the proximal ulna.
- No elongation or foreshortening of the humeral epicondyles.
- Partially open elbow joint if the shoulder was placed in the same plane as the forearm.
- Similar radiographic densities of the proximal and distal forearm.
 |
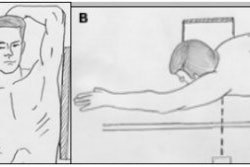
Positioning for a lateral projection of the forearm
- Seat the patient close to the radiographic table and low enough so that the humerus, shoulder joint, and elbow lie in the same plane.
- Flex the elbow 90º, and center the forearm over the unmasked half of the cassette and parallel with the long axis of the forearm.
- Make sure that the entire joint of interest is included.
- Adjust the limb in a true lateral position; the thumb side of the hand must be up.
- The CR is perpendicular to the midpoint of the forearm.
Evaluation criteria
- Lateral projection of the entire radius and ulna along with wrist and distal humerus should be clearly demonstrated.
- No rotation as evidenced by:
- Superimposition of the radius and ulna at their distal end.
- Superimposition by the radial head over the coronoid process.
- Radial tuberosity facing anteriorly.
- Superimposed humeral epicondyles.
- Elbow should be flexed 90º.
- Pertinent soft tissues, such as fat pads and stripes of the wrist and elbow joints, and bony trabeculations should be visible.
 |
Radiographic positioning of the elbow
Routine radiographic examination of elbow is performed using the AP, AP oblique, and lateral projections. AP oblique projections include medial (internal) rotation and lateral (external) rotation views.
The lateral projection (lateromedial view) is obtained by flexing the elbow 90º. Diagnosis of certain important joint pathological processes (such as possible visualization of the posterior fat pad) depends on 90º flexion of the elbow joint. By doing this, the olecranon process can be seen in profile, and the elbow fat pads are the least compressed. Also, by allowing a partial or complete extension, the olecranon process elevates the posterior elbow fat pad and simulates joint pathology.
Technical factors
- IR: Lengthwise 11 x 14 inch (30 x 35 cm) divided; 7 x 17 inch (18 x 43 cm) single; 14 x 17 inch ( 35 x 43 cm) divided.
- Detail screen, tabletop.
- 60 to 65 kVp range, mAs 6.
- Minimum SID of 100 cm.
 |
Positioning for an AP projection
- Seat the patient near the radiographic table and low enough to place the shoulder joint, humerus, and elbow joint in the same plane.
- Extend the elbow, supinate the hand.
- When the elbow cannot be fully extended, obtain two AP projections -- one with forearm parallel to IR and one with humerus parallel to IR.
- Center the cassette to the elbow joint.
- Adjust the cassette to make it parallel with the long axis of the arm.
- Ask the patient to lean laterally until the humeral epicondyles and anterior surface of the elbow are parallel with the plane of the cassette.
- Supinate the hand to prevent rotation of the bones of the forearm.
- The CR should be perpendicular to the elbow joint.
Evaluation criteria
- Distal humerus, elbow joint space, proximal radius, and ulna should be clearly demonstrated.
- No rotation is evidenced by appearance of bilateral epicondyles seen in profile; radial head, neck, and tuberosity slightly superimposed over the proximal ulna.
- Elbow joint appears open with fully extended arm.
- Soft tissue and bony trabeculation should be visible.
 |
Positioning for a lateral projection
- Seat the patient at the end of the radiographic table low enough to place the humerus and elbow joint in the same plane with elbow flexed 90º.
- Align long axis of the forearm to the long axis of the cassette.
- Place the humerus and forearm in contact with the table.
- Center the cassette to the elbow joint.
- Adjust the cassette diagonally to include most of the arm and forearm.
- Rotate the hand and wrist in to a true lateral position, thumb side up, and ensure that the humeral epicondyles are perpendicular to the plane of the cassette.
- The CR should be perpendicular to the elbow joint, regardless of its location on the cassette.
Evaluation criteria
- Distal humerus, proximal forearm should be clearly demonstrated.
- Open elbow joint centered to the central ray.
- Elbow flexed 90º.
- Superimposed humeral epicondyles.
- Radial tuberosity facing anteriorly.
- Radial head partially superimposing the coronoid process.
- Olecranon process seen in profile.
- A true lateral projection is indicated by three concentric arcs of the trochlear sulcus, double ridges of the capitulum and trochlea, and the trochlear notch of the ulna.
- Bony trabeculation and any elevated fat pads in the soft tissue at the anterior and posterior distal humerus and the anterior proximal forearm should be visible.
 |
Positioning for an AP oblique projection medial (internal) rotation
- Seat the patient at the end of the radiographic table with the arm extended and in contact with the table.
- Extend the limb in position for an AP projection, and center the midpoint of the cassette to the elbow joint.
- Medially (internally) rotate or pronate (palm-down) the hand.
- Adjust the elbow to place its anterior surface at an angle of 45º (palpating epicondyles to determine a 45º rotation). This degree of obliquity usually clears the coronoid process of the radial head.
- The CR should be perpendicular to the elbow joint.
Evaluation criteria
- Coronoid process in profile should be clearly demonstrated.
- Elongated medial humeral epicondyle.
- Ulna superimposed by the radial head and neck.
- Olecranon process within the olecranon fossa.
- Soft tissue and bony trabeculation visible.
 |
Positioning for an AP oblique projection lateral (external) rotation
- After seating the patient at the end of table, extend the patient's arms into position for an AP projection.
- Center the midpoint of the cassette to the elbow joint.
- Rotate the hand laterally (externally) to place the posterior surface of the elbow at a 45º angle.
- When proper lateral rotation is achieved, the patient’s first and second digits should touch the table.
- The CR should be perpendicular to the elbow joint.
Evaluation criteria
- An oblique view of the distal humerus and proximal radius and ulna should be demonstrated.
- Correct 45º lateral oblique should project the radial head, neck, and tuberosity, free of superimposition by ulna.
- Open elbow joint should be clearly demonstrated.
- Soft tissue and bony trabeculation should be visible.
AuntMinnie.com contributing writer
November 21, 2002
Related Reading
The twists and turns of hand and wrist x-ray positioning, October 15, 2002
Digit imaging requires diligent positioning, September 17, 2002
Patient positioning techniques for a lower gastrointestinal series, June 27, 2002
Patient positioning tips for a premium UGI series, April 17, 2002
Positioning techniques for quality esophagrams, March 20, 2002
Copyright © 2002 AuntMinnie.com