Stereotactic radiosurgery appears superior to endovascular embolization for treating patients with eloquent brain arteriovenous malformations (AVMs), according to a study published October 21 in Radiology.
The finding is from among the first direct comparisons of the two minimally invasive techniques for treating brain AVMs, which are uncommon tangles of arteries and veins, noted lead author Basel Musmar, MD, of Thomas Jefferson University Hospital in Philadelphia, and colleagues. ("Eloquent" brain areas are those critical for essential functions such as motor, sensory, or language processing.)
“Stereotactic radiosurgery was associated with a higher obliteration rate compared with embolization in patients with eloquent brain arteriovenous malformations,” the researchers wrote.
An AVM is a tangle of blood vessels that creates irregular connections between arteries and veins, typically in the brain, the authors explained. If an AVM bursts, it can cause bleeding and lead to a stroke or brain damage. The primary goal of AVM treatment is to completely obliterate the tangle to eliminate the risk of hemorrhage, the team noted.
While surgical resection is the definitive treatment, its risks are amplified for AVMs in eloquent brain areas. Conversely, stereotactic radiosurgery and endovascular embolization increasingly are being used, yet no studies to date have directly compared patient outcomes from the emerging techniques, according to the group.
To address the knowledge gap, the group assessed the success of the procedures among 119 patients (median age, 35; 64 female): 96 patients were treated with stereotactic radiosurgery and 23 with embolization. They used pre- and post-treatment digital subtraction arterial angiography, MR angiography, or CT angiography to directly compare outcomes and propensity score weighting (PSW) to make up for differences in the two groups.
 Digital subtraction angiography images in a 65-year-old female patient with a right thalamic arteriovenous malformation (AVM). (A) Lateral digital subtraction angiography image of the right internal carotid artery in the arterial phase shows a compact AVM nidus located in the right posterior thalamus, supplied by distal branches of the posterior cerebral artery via a fetal-type posterior cerebral circulation. (B) Anteroposterior digital subtraction angiography image from the same diagnostic angiogram demonstrates deep venous drainage. The patient underwent Gamma Knife (Elekta) stereotactic radiosurgery four months later, with a single-fraction dose of 20 Gy using cobalt 60 energy, prescribed to the 68% isodose line across 14 shots. (C) Lateral digital subtraction angiography image at 3-year follow-up shows no residual arteriovenous shunting, consistent with complete angiographic obliteration. (D) Corresponding anteroposterior digital subtraction angiography image at the same time point confirms durable obliteration. Iodinated contrast agent (Omnipaque, GE HealthCare) was used for all angiographic acquisitions.RSNA
Digital subtraction angiography images in a 65-year-old female patient with a right thalamic arteriovenous malformation (AVM). (A) Lateral digital subtraction angiography image of the right internal carotid artery in the arterial phase shows a compact AVM nidus located in the right posterior thalamus, supplied by distal branches of the posterior cerebral artery via a fetal-type posterior cerebral circulation. (B) Anteroposterior digital subtraction angiography image from the same diagnostic angiogram demonstrates deep venous drainage. The patient underwent Gamma Knife (Elekta) stereotactic radiosurgery four months later, with a single-fraction dose of 20 Gy using cobalt 60 energy, prescribed to the 68% isodose line across 14 shots. (C) Lateral digital subtraction angiography image at 3-year follow-up shows no residual arteriovenous shunting, consistent with complete angiographic obliteration. (D) Corresponding anteroposterior digital subtraction angiography image at the same time point confirms durable obliteration. Iodinated contrast agent (Omnipaque, GE HealthCare) was used for all angiographic acquisitions.RSNA
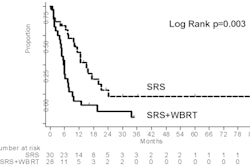
According to the results, at last follow-up, stereotactic radiosurgery (SRS) achieved complete obliteration of AVMs in 61 of 86 patients (71%) compared with 10 of 18 patients (56%) in the embolization group. The SRS group also had higher rates of modified Rankin Scale scores 0-2 at last follow-up (95% [86 of 91 patients] vs. 71% [15 of 21 patients]), the researchers reported.
In addition, the SRS group had a lower rate of hemorrhagic complications (5.2% [5 of 96 patients] vs. 26% [6 of 23 patients]) compared with the embolization group, while mortality rates were 2.1% (2 of 96) in the SRS group and 4.3% (1 of 23) in the embolization group.
“These findings indicate that SRS provides superior angiographic efficacy without compromising clinical safety in eloquent AVMs,” the researchers wrote.
Ultimately, future research is warranted to validate these results and further optimize treatment strategies for this challenging patient population, the group concluded.
In an accompanying editorial, Eric Russell, MD, of Northwestern University in Chicago, wrote that the results certainly favor the use of SRS for AVMs in eloquent locations, yet echoed that further analysis is warranted.
“Decisions will continue to be individualized given variabilities in angioarchitecture, specific location, and local expertise and experience,” he wrote.
For instance, embolization may be a better option for patients with significant neurologic deficits or urgent clinical indications, with literature also supporting its use for small to medium superficial lesions with compact nidal architecture. Ultimately, there is no single winner of the race to cure brain AVMs in eloquent areas, Russell wrote.
“Ongoing improvements with each strategy will continue to evolve and influence decision-making,” he concluded.
The full study is available here.