SAN FRANCISCO - A streamlined protocol for breast MRI could make the modality a viable option for breast cancer screening by cutting image acquisition and reading time to just three minutes, according to a presentation on September 7 at the American Society of Clinical Oncology (ASCO) 2013 Breast Cancer Symposium (BCS).
Current breast MRI protocols are designed for diagnostic rather than screening purposes and are therefore time-consuming to acquire and read -- which contributes to the modality's relatively higher cost and limited availability, said presenter Dr. Christiane Kuhl, of the University of Aachen in Germany.
Kuhl and colleagues investigated whether a streamlined protocol, consisting only of the first postcontrast subtracted images and their maximum intensity projection (MIP) reconstructions, would be suitable for screening purposes. The idea was to trade some of the high sensitivity of breast MRI for acquisition and interpretation speed, with a long-term goal of increasing access to breast MRI by reducing the cost associated with the examination, according to Kuhl.
 Dr. Christiane Kuhl, from the University of Aachen in Germany.
Dr. Christiane Kuhl, from the University of Aachen in Germany.
"We conducted this proof-of-concept study to explore whether we could use MRI as a real breast cancer screening tool by reducing the acquisition and reading time," Kuhl said. "A full breast MRI imaging protocol is 21 minutes. We cut everything away and reduced the time to three minutes."
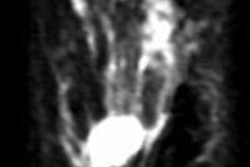
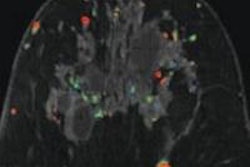
Kuhl and colleagues tested the protocol in a population of 443 women at increased risk of breast cancer who had undergone 606 breast MRI screening studies. Images were read by experienced breast radiologists who were asked to first review the MIPs and search for significant enhancement, and then to evaluate the first postcontrast subtracted images for any further categorization. (The first postcontrast subtracted images show the change in image due to contrast; MIP is a volume rendering method for 3D data.)
After the radiologists had read images produced with the streamlined protocol, they then analyzed the full diagnostic breast MRI protocol. Kuhl's group then compared the diagnostic yield and accuracy of the streamlined readings versus that of the full protocol.
Kuhl's team found that the average time required to read MIPs was 2.8 seconds, while 28 seconds were required for the postcontrast subtracted images. Patient setup consumed the rest of the time required for the three-minute protocol. A total of 11 breast cancers were diagnosed, for an additional yield of 18.2 cancers per 1,000 women.
Of these cancers, four were ductal carcinoma in situ (DCIS) and seven were invasive, with a median size of 8 mm. All were intermediate or high grade. The streamlined protocol detected nine (82%) of the 11 cancers; specificity of the protocol was the same as that of the full protocol, at 94.4%. The streamlined protocol had 33 false-positive diagnoses, versus 35 for the full procedure.
The negative predictive value of the streamlined protocol was 99.6%, compared with 99.8% for the full protocol, according to the researchers.
"This abridged protocol allowed for a substantial additional yield of biologically relevant, invasive cancers and DCIS in a cohort of women with slightly or moderate increased risk of breast cancer," Kuhl said.
MRI offers something that mammography does not, according to Kuhl: Sensitivity to biologically active disease.
"As a technology, mammography has an inherent bias to detect slow-growing cancers," Kuhl told session attendees. "It's based on architectural distortions, spiculations, and calcifications -- it reflects regressive changes. In contrast, MRI detects cancers that are biologically active, characterized by angiogenic and protease activity."
In the context of the ongoing debate about the overdiagnosis of breast cancer, is it a good idea to look for new screening tools? Yes, Kuhl said, and it's important not to confuse finding more cancers with overdiagnosis.
"Very simply, too many women continue to die of breast cancer," she said. "The aim of nonmammography screening strategies is to find the right cancers -- the ones that kill."