Clinicians should be able to avoid the use of gadolinium-based contrast agents (GBCAs) on follow-up MRI brain scans to accurately monitor disease progression in patients with multiple sclerosis (MS), according to a study published online March 12 in Radiology.
Using 3-tesla MRI and current protocols, German researchers missed less than 1% of new or enlarged lesions on more than 500 nonenhanced follow-up MR images in a direct comparison with matching GBCA-enhanced MR images. In other words, the use of a GBCA for MRI follow-up did not change the diagnosis of interval disease progression in MS patients (Radiology, March 12, 2019).
"Our data do not support the notion that the use of contrast material results in higher sensitivity for the detection of new or enlarged lesions in MS compared with unenhanced MRI at 3T," wrote lead author Dr. Paul Eichinger and colleagues from the Technical University of Munich in Germany.
Why MRI?
MRI has proved particularly adept at detecting newly recurring inflammatory lesions related to multiple sclerosis, which in turn indicate disease activity or progression. This occurrence is one reason why MS patients undergo periodic follow-up 3-tesla MRI exams with the addition of sequences such as 3D isotropic, double inversion recovery (DIR), and fluid-attenuated inversion recovery (FLAIR) to better visualize abnormalities in the brain. The DIR sequence, in particular, is well-known for its ability to detect cortical and white-matter lesions.
"Recently, longitudinal subtraction techniques have been developed that show new or enlarged lesions as bright spots while pre-existing lesions and normal-appearing brain parenchyma are canceled out," the researchers noted. "Such techniques substantially improve the sensitivity in the detection of new or enlarged lesions in MS at follow-up imaging."
Given the availabilities of these tools, Eichinger and colleagues questioned whether gadolinium contrast is necessary to enhance the detection of new or enlarged lesions on follow-up MRI scans. The ability to avoid administering contrast to MS patients could be worthwhile in light of recent research and the debate over the effects of gadolinium retention in the brain and other body regions years after an MRI scan.
"These factors warrant evaluation of strategies for reducing or omitting contrast agent, especially in MS patients who often accumulate a high number of MRI scans over their lifetimes," added senior author Dr. Benedikt Wiestler in a statement.
With and without contrast
To compare the options, the researchers performed a retrospective study that included 359 patients (mean age at baseline, 38.2 ± 10.3 years) who underwent MRI scans on a 3-tesla system (Achieva, Philips Healthcare) between January 2014 and December 2016. The MRI protocol consisted of 3D FLAIR, 3D DIR, and 3D T1-weighted sequences before and at least five minutes after administration of 0.1 mmol/kg gadolinium-based contrast (Dotarem, Guerbet). The scans produced 507 pairs of baseline and follow-up MR images, with time between the scans ranging from one month to more than two years.
The researchers also added longitudinal subtraction maps to detect new or enlarged MS lesions because the maps are "easy to calculate, requiring only the coregistration of images, and have a high lesion-to-background ratio. In addition, these maps help identify changes in size (and shape) of pre-existing lesions, further increasing the sensitivity in the detection of interval progression," they explained.
As it turned out, the combination of DIR and subtraction maps with nonenhanced MR images was most successful in identifying a total of 1,992 new or enlarged lesions on 264 (52%) of the 507 follow-up MR images, compared with 207 (41%) contrast-enhanced MR images that uncovered new or enlarged lesions.
Four of the 1,992 lesions were detected later only on the nonenhanced images, meaning that the researchers initially missed a mere 0.2% of abnormalities without the use of contrast.
Of the 207 contrast-enhanced detected lesions, 203 (98%) of them were seen as new or enlarged lesions on nonenhanced MR images together with the DIR-subtraction map approach. The contrast-enhanced image sequences did not find any disease progression on any of the 507 images that went undetected by nonenhanced MRI sequences with either DIR- or FLAIR-based subtraction maps.
One other finding of note was that FLAIR with subtraction maps was not as proficient as the DIR-subtraction map approach. FLAIR with subtraction maps observed a total of 1,442 lesions, 27% fewer than DIR with subtraction maps.
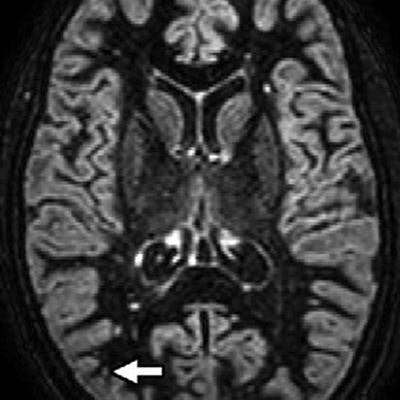
 Axial MR images come from a 32-year-old woman with relapsing-remitting multiple sclerosis. Images were obtained with the subtraction of an unenhanced T1-weighted MR image from contrast-enhanced MR image (T1sub), FLAIR, and DIR. A new small subcortical lesion (arrow) in the right parietal lobe is seen only on the contrast-enhanced image but is overlooked on DIR and FLAIR sequences. There are several other new or enlarged lesions that can be seen on nonenhanced images. Images courtesy of Radiology.
Axial MR images come from a 32-year-old woman with relapsing-remitting multiple sclerosis. Images were obtained with the subtraction of an unenhanced T1-weighted MR image from contrast-enhanced MR image (T1sub), FLAIR, and DIR. A new small subcortical lesion (arrow) in the right parietal lobe is seen only on the contrast-enhanced image but is overlooked on DIR and FLAIR sequences. There are several other new or enlarged lesions that can be seen on nonenhanced images. Images courtesy of Radiology."In our cohort, contrast-enhanced T1-weighted MRI provided no benefit at a per-patient level over longitudinal subtraction maps obtained from nonenhanced sequences for detecting new or enlarged lesions in 507 follow-up examinations of patients with MS," Eichinger and colleagues concluded. "In no case was interval progression missed when only nonenhanced sequences were analyzed. On a per-lesion basis, less than 1% of new or enlarged lesions were overlooked when only nonenhanced sequences were analyzed."
While the findings are impressive using 3-tesla MRI with 3D sequences and no contrast, the researchers acknowledged that it is "unclear" whether the same results could be accomplished with 1.5-tesla MRI and/or 2D sequences.
"Our data support the view that modern 3D sequences at 3T in combination with image subtraction are ready to supersede routine use of contrast material in most instances of follow-up investigations of patients with MS, reducing both imaging time and cost without missing new or enlarged lesions," Eichinger and colleagues wrote.