County-level "social capital" -- that is, a set of shared values or resources that enables people to work together in a group to achieve a common goal -- is linked to higher screening mammography rates, researchers have reported.
Regarding social capital, community and institutional health indices and nonmetropolitan areas were associated with higher mammography rates, according to the report led by Tracy Huang and Christine Ekenga from Emory University in Atlanta, GA. Their study results were published March 4 in Preventive Medicine Reports.
“These findings suggest that enhancing public trust and community engagement may improve screening behaviors,” Huang and Ekenga wrote.
Previous studies suggest that social capital enhances mutual support among communities, which can lead to improved health, and specifically for screening mammography, research has suggested that individual-level social capital is positively tied to higher mammography rates.
Huang and Ekenga studied the relationship between social capital and mammography screening rates among older U.S. women via an analysis that included data from 2,765 U.S. counties consisting of 2018 county-level screening mammography rates among female Medicare enrollees ages 67 to 69. The team obtained social capital information from the 2018 Social Capital Project, including indices for family unity, institutional health, collective efficacy, and community health.
The team categorized these indices into four groups based on quartile values. These included the following: The fourth group (Q4), which represented counties with values above the 75th percentile; the third group (Q3), which included counties with values between the median and the 75th percentile; the second group (Q2), which comprised counties with values between the 25th percentile and the median; and the first group (Q1), which represented counties with values below the 25th percentile.
Among the counties included, mammography screening rates ranged from 17% to 64%, with an average of 41%.
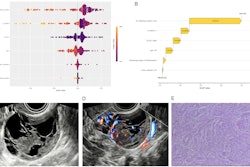
The researchers identified the following strong positive associations between the following: social capital and mammography rates (Q4 vs. Q1: adjusted prevalence ratio [aPR] = 2.29, with 1 as reference); community health index (Q4 versus Q1: aPR = 1.99; and institutional health index (Q4 versus Q1: aPR = 4.31).
Huang and Ekenga noted that these associations were strongest among nonmetropolitan counties. Finally, they found no significant associations for family unity or collective efficacy.
For the community health index, the team highlighted that this trend may be due to involvement in community and religious activities that improve health awareness, increase access to resources, and provide social support for health-promoting behaviors. For the institutional health index, they wrote that this may be explained by the idea that people who don’t have public trust in institutions would be less likely to trust medical advice and adhere to recommended screening guidelines set by agencies that receive support from governmental institutions.
Huang and Ekenga called for future studies to investigate social capital domains at the individual, neighborhood, and county levels to understand their impact on mammography screening.
“While this study specifically focused on mammography rates, future studies are warranted to examine social capital's role across various screening behaviors for different cancers,” they added.
The full study can be found here.