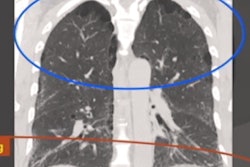
Volumetric analysis of lung consolidation on chest CT scans can be used to predict the risk of COVID-19 patients dying in the hospital and aid in management decisions, researchers from Michigan reported in a study published online January 6 in European Journal of Radiology Open.
Using radiation therapy planning software, a group led by Dr. Lucas Sapienza of Michigan State University in Southfield, MI, assessed the impact of lung involvement on clinical outcomes in over 150 COVID-19 pneumonia cases. They found that each unit percentage of lung involvement by consolidations resulted in increased risk of in-hospital mortality, as well as higher probability of major adverse hospitalization events.
"[T]his study provides evidence that chest CT is a potential tool in guiding escalation or de-escalation of care in the hospital setting," the authors wrote.
The researchers hypothesized that by proportionally reflecting lung parenchyma involvement, the quantity of opacities relative to the total lung volume may be predictive of survival and the need for more intensive medical care.
To test this hypothesis, they performed a volumetric analysis of lung opacities in the chest CT exams of 154 COVID-19 patients at their institution between February and April 2020 and evaluated the association of relative lung involvement with outcomes. These patients had a median lung involvement of 28.8%; 36 (26.3%) were intubated and 25 (16.2%) died in the hospital.
The researchers used version 15.6 of the Eclipse radiotherapy planning software (Varian Medical Systems) to perform volumetric analysis of images from the patients' initial CT exams.
"We choose radiation oncology software due to the enhanced structure delineation capability in three planes (axial, coronal, and sagittal), real-time tridimensional reconstruction, and the precision of the volumetric measurement tools," they wrote.
Two radiation oncologists with five- and 10-years' experience, respectively, performed contours of the lungs and the consolidations. The researchers then calculated the relative consolidation volume by dividing the volume of the lung consolidations by the total bilateral lung volume.
After performing multivariate logistic regression analysis and adjusting for significant clinical factors, the researchers found that each percentage unit of lung involvement led to a 3.6% increased risk of in-hospital mortality and a 2.5% higher risk of major adverse hospitalization events.
Other factors associated with increased in-hospital mortality risk included advanced age (p = 0.013), do not resuscitate/do not intubate status at admission (p < 0.001), and smoking (p = 0.008). As for risk of major adverse hospitalization rates, older patients (p = 0.032) and males (p = 0.026) had higher probabilities, according to the authors.
According to the findings, a patient who is older than 65 years of age and has a history of smoking has a 15% risk of dying during hospitalization if 10% of the lung is involved at the initial assessment. This risk would grow to 50% for a similar patient with 60% of lung involvement.
"Important information to better predict prognosis and guide clinical management can be derived from our findings," the authors wrote.