Researchers in Austria have developed a CAD system to detect metacarpal bone-contour defects associated with rheumatoid arthritis. The prototype system was fast, and highly accurate, in a preliminary study aimed at comparing CAD’s performance with that of experienced musculoskeletal radiologists.
"The experience, skill, and aptitude of the individual rating the abnormalities are major determining factors" affecting the accuracy of contour-abnormality detection, said Dr. Philipp Peloschek from the Universitätsklinik für Radiodiagnostik at the University of Austria.
Even a reduction of reading time to 3-4 minutes (from the current 6-8 minutes) would be a major accomplishment, he said, but attempts to do so at his institution have produced inconsistent results, inspiring the effort to develop RheumaCoach CAD (Annals of the Rheumatic Diseases, June 2003, Vol. 62:6, pp. 579-582).
The latest study, presented by Peloschek at the 2004 European Congress of Radiology in Vienna, examined the system’s performance in 10 patients.
Snake algorithms and erosion detection
The CAD software, which runs on any laptop computer, relies on a database that was acquired from the x-ray images of 30 normal subjects. The first automated task is bone-contour detection, which estimates the shape of the patient’s metacarpal bones based on a normative database or template. Then the algorithm adapts the template to the individual image based on anatomic landmarks. Finally, bone contour is estimated via a mathematical formula, deciding yes or no if there is erosion, and then marking any perceived deformities for the radiologist’s review.
 |
| The yellow dashed line indicates first approximation of the bone contour by an active shape model (ASM), "ignoring" everything that does not fit into the ASM, which has been trained only on intact bones. The line with red dots indicates the "ASM-driven snake" result. A more flexible search is started from the first ASM approximation (dashed line) and adapts also to erosions and fine structure on the bone contour. All images courtesy of Dr. Philipp Peloschek. |
"The 'ASM-driven snakes' algorithm is based on an initialization by active shape models (ASM)," Peloschek explained in an e-mail to AuntMinnie.com. "These models … contain ‘knowledge’ about the variability of bone shapes. Thereby they are able to detect the bone contour with high robustness and reasonable accuracy."
 |
| Above, erosion at fifth MCP joint. Below, red line indicates the result of the automated joint-contour detection algorithm, which adapts also to erosions and fine individual structures of the bone contour. |
 |
Another step is needed to deal with anatomical variation and pathological deformations of bones, Peloschek said, meaning that the ASM results can be used only as a rough first approximation. The additional precision is obtained with initialization of a "snake algorithm" (aka the "rubber band"), which moves about more freely than the ASM throughout the image domain.
By controlling parameters such as the elasticity and rigidity of the snake, the snake algorithm adapts the bone-contour estimate to the real bone boundary, even in areas where the bone contour has been affected by rheumatoid arthritis. Still, the snake algorithm is a work-in-progress. There are no erosions in the normative dataset, so these variations cannot be modeled by the ASM, he said.
Preliminary study
In their study, Peloschek, along with Georg Langs, a mathematician from the pattern recognition and image processing group at Vienna University of Technology; Horst Bischof, Ph.D. from Graz University of Technology; and Franz Kainberger, Ph.D. from Vienna Medical University, applied the CAD algorithm in radiographs of 10 patients.
CAD localization was performed on the carpometacarpal, metacarpophalangeal, and distal interphalangeal bones of 10 patients in 10 radiographs, using 42 landmarks per metacarpal bone for a total of 420 measurements. The results were then analyzed statistically.
An automatic feature-selection process showed preference for the same signs used by radiologists, for example, concavity and rough or soft delineation of the contour. Preliminary experiments on the small dataset used in the study showed an approximate 4% error rate, Peloschek said; experiments with different classifiers are still underway.
Additional image processing demonstrated the robustness of the CAD localizer process, which yielded a mean position error of 2.7 mm, as well as high accuracy for the detection of bone contours. The median error orthogonal to the contour was 0.113 mm, and 74.6% of the landmarks in the test set were within a 0.25-mm window of error. The entire process takes about 30 seconds per study, Peloschek said.
CAD produced an accurate parametrical description of the identified shape, he concluded, noting that additional research will be required to determine the CAD’s ability to accurately assess bone erosion by means of mathematical extraction of the data. The issues of bone rotation and bone-texture evaluation are also in line for development work.
Slides depicting two CAD misreads, including a stretched metacarpal bone that resulted in a false-positive call for impact bone erosion, and an erosion that was missed entirely, spoke to the need for further refinement. "Altogether I think we’re going in the right direction," Peloschek said.
"We have a very precise localizing procedure for the estimation of the bony contour that has a very low perpendicular error," he said. "The most important thing is that each of our steps is precise enough to enable the succeeding algorithms to rely on them."
 |
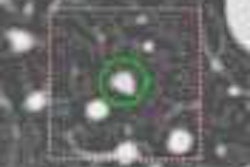
| The CAD algorithm has recently been configured to measure joint spaces. Above, fifth metacarpal bone of a 20-year-old woman with recently diagnosed rheumatoid arthritis. This joint is not affected by the disease. The thin dashed red and blue lines indicate the ASM results of the bone contours. The joint space width is measured as mean distance between the green lines: Here the calculated joint space width was about 1.9 mm. |
The group is currently looking for development partners, and eventually plans to roll out a kind of automated teleradiology service for the DICOM-compliant CAD system. Radiologist would use the service by sending image data over the Internet to the CAD on a central server, and having the computer send its opinions back to them quickly.
By Eric BarnesAuntMinnie.com staff writer
May 18, 2004
Related Reading
Wrist MRI predicts functional outcome in early rheumatoid arthritis, April 30, 2004
Portable MRI better than x-ray at detecting inflammatory arthritis, April 27, 2004
Risk of vertebral deformities increased in women with RA, March 8, 2004
Copyright © 2004 AuntMinnie.com