Part 2 of our series on the Eugene P. Pendergrass New Horizons Lectures at the 2012 RSNA meeting covers Dr. Paul Chang's lecture on how medical imaging IT can ensure that radiologists thrive in the new era of healthcare. Click here for Part 1, which covers a presentation by Dr. Keith Dreyer, PhD, on the future of radiology informatics.
CHICAGO - To recapture their role as the "doctor's doctor," radiologists must be value innovators, said Dr. Paul Chang of the University of Chicago School of Medicine. Advances in information technology will be crucial for the specialty to demonstrate value and avoid commoditization.
"We have to become irreplaceable and add measurable, demonstrable, and differentiable value to our clinical colleagues in this aligned environment," said Chang, a professor and vice chair of radiology informatics.
In the old days before PACS, the radiologist was once considered to be the "doctor's doctor," with medical and surgical rounds starting in radiology in the morning. That's no longer the case, however, and the primary technology that has facilitated radiology commoditization and outsourcing is digital image management, Chang said.
 Dr. Paul Chang, from the University of Chicago.
Dr. Paul Chang, from the University of Chicago.
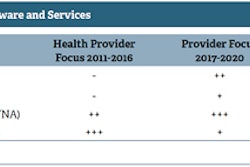
In the first generation of PACS, the focus was on getting rid of film and had a radiology-centric emphasis. This filmless goal was achieved and we're now in the sunset phase of the second generation of PACS, which has revolved around workflow and an enterprise-centric vision that encompassed other specialties such as cardiology and pathology, he said.
This included utilizing technology such as the Web, thin clients, mobile devices, and the cloud, Chang said. The problem, though, is that the emphasis was still on the images and the ability to ubiquitously distribute and access those images. There wasn't a lot of discussion about the value-add for the radiologist.
"If anything, it actually dissuaded the collaboration," he said. "I could sit in the reading room, my surgical colleague could be in the OR or the clinic, and rarely would we interact. How easy is it, then, to be commoditized or devalued in that environment where we don't see each other or we don't collaborate?"
PACS 3.0
Chang believes we are now embarking on the next generation of PACS or radiology IT. This generation will focus on meaningful innovation for meaningful use, moving beyond the enterprise to the cloud, emphasizing the value proposition for radiologists, and navigating disruption, Chang said.
"Our responsibilities, our stakeholders, are not just within our firewall," he said. "They are beyond our enterprise ... we're going to be responsible for being able to add value, provide images, our interpretations, our collaborative skills beyond our enterprise to where the patients live, to where our health consumers live."
The emphasis will be on demonstrating true, differentiable value, and it will require the use of tools to navigate this disruptive time where there will be a shift from a predominantly fee-for-service model to a more aligned approach.
"Whether or not there are truly accountable care organizations, I think it's already too late to hope that those go away," he said. "I think that no matter what happens it will be more of an aligned model."
Medical imaging is currently stuck between a rock and a hard place, with market drivers encouraging commoditization on one hand and the demand for improved and demonstrated value on the other, Chang said.
Reimbursements will continue to decrease, and consolidation and competition will also only increase. At the same time, healthcare reform and the move toward accountable care organizations (ACOs) are driving a shift toward alignment as a new healthcare delivery model, Chang said. Improvements must be realized in efficiency, quality, and safety.
"Whatever your utility function is, that utility function has to be optimized not only for radiology, but for your aligned colleagues as well -- the entire enterprise," he said. "This is a challenge for us and this is something where I think IT can play a helpful role."
The traditional fee-for-service model may be inconsistent with these new alignment models, and the commoditization of radiology services is a true risk, Chang said.
But there are also opportunities. Radiologists will no longer be valued just for interpreting images; instead, they will be valued for managing the role of imaging in a capitated, aligned system, he said.
"We have to be perceived as irreplaceable in this aligned model and have to provide evidence ... and demonstrate to that aligned enterprise that we truly add value," Chang said. "In other words, we need to be a differentiable value innovator."
Value
Value in medical imaging is some function of quality, efficiency, and safety, Chang said. While radiology could get away in the past with optimizing one of these three variables, all three must now be delivered to demonstrate value.
"We need IT and informatics solutions that provide meaningful innovation to allow us to maximize value, simultaneously optimizing quality, efficiency, and safety so as to demonstrate measurable value to our patients," he said.
The common belief that PACS is a "solved" technology is a misconception. In fact, Chang believes that the immaturity of the existing radiology IT and informatics offerings has actually allowed radiology to only demonstrate commodity-level service.
"They do not allow us to differentiate ourselves, to demonstrate my differentiable value relative to another competitor," he said. "We require significantly more capable and agile IT solutions to provide measurable value to patient care in an environment that is much more complex and competitive."
Meaningful IT innovation
Chang said that meaningful IT innovation can be achieved in four areas:
- Advanced workflow to support enterprise-wide value
- "Comprehensive" collaboration
- Business intelligence and analytics
- Connecting with the health consumer
Advanced workflow to support enterprise-wide value requires optimizing information throughput and quality throughout the enterprise, he said.
"We have to get away from the reading-room-centric bias that what's good for the radiologist is what's good for everybody else," he said. "We have to embrace meaningful innovation in that whatever we do propagates upstream and downstream efficiency and quality throughout the enterprise in this aligned model, whatever it might become in the future. This is important because that's how you become irreplaceable."
The same technology and integration approaches that have been successful in the reading room must be applied throughout the enterprise, he said.
Traditional radiology department measures such as patient throughput and report turnaround times are insufficient; improved information throughput is the real goal, Chang said.
"The clock doesn't start in radiology; the clock starts with the patient and a physician, where the physician may believe an imaging study may be contributory to the management of her patient and only ends when that same physician gets a collaborative message from me," he said.
For example, the University of Chicago utilizes a concept it calls Closed Loop Imaging, in which the clock starts with the patient.
Chang also cited examples such as Massachusetts General Hospital's use of computerized physician order entry (CPOE) and providing appropriateness criteria to ordering physicians.
Advanced imaging electronic protocol tools would be valuable, and also allow for extension of integration and interoperability to the modality itself, he said. The University of Chicago has realized 66% to 70% improvement in CT scanner cycle time by automating procedures that were originally done by humans; these procedures can be done more rapidly and more efficiently electronically with integration, he said.
Another possible example is a tool such as Lesion Tracker Intelligent Agent, an early Philips Healthcare/University of Chicago research prototype that automates tracking of lesion measurements for oncology. Mean measurement reporting time per lesion was reduced by almost 50%, but more importantly, efficiency and accuracy were also improved downstream for the oncologist, Chang said.
Collaboration
Comprehensive collaboration means going beyond the report and the phone call, Chang said. He noted that the youth of today use a wide variety of virtual collaborative tools such as Twitter, Foursquare, Facebook, Skype, YouTube, SMS, etc., and can articulate intelligently why they need all of those mediums.
"As a radiologist, I basically have the report and a phone call," he said. "We've got to do better."
To move from communication to true collaboration, radiologists must move from the Web 1.0 passive consumption model to Web 2.0, which emphasizes collaboration and active participation with the use of virtual collaborative tools, Chang said.
"Our kids foster the Web to facilitate shared context to support virtual collaboration, where content and the sharing of content and the consumption of content and the creation of content are intermixed," he said. "That's what it used to be when the clinicians came to us in the morning to collaborate."
For example, multimedia reports can, via progressive disclosure, provide greater detail on the meaning of findings, he said. Multimedia reporting tools available in the market today can create multimedia reports faster than a static report.
"Value is optimized, [as well as] quality and efficiency," he said.
The radiology report should be viewed as a portal, he added. "In other words, instead of statically saying I used this much of contrast, use it as a hyperlink. Most of our physicians are going to consume these electronically anyway."
Business analytics
Business analytics is 10 years behind in radiology, Chang said.
"We have to go beyond monthly reports and have to go beyond fancy little dashboards and widgets," he said. "The emphasis is on intelligence; we want real-time tactical agents, dashboards, and strategic scorecards against key performance indicators."
This requires intelligent dashboards that automatically use natural language processing to extract information from the electronic medical record (EMR) to gain clinical context without wasting five or 10 minutes to go to the EMR, he said.
Tools are needed to correlate indications with findings and outcomes, according to Chang.
"In order to do that, we need integration and interoperability to feed our analytics engines from sources that go beyond radiology," he said.
Connecting to consumers
Patients are now discriminating health consumers with rapid access to information and expectations for service quality, he said.
Meeting these expectations requires better integration, orchestration rather than choreography, and an enterprise perspective. Technically, this isn't that difficult a task.
"The real challenge is changing ourselves," he said. "Understanding that whatever we do, we have to get beyond optimizing the reading room, optimizing the radiology experience."