Substantial regional variations in imaging utilization rates exist across the U.S., but the differences are not as high as reported in previous studies, according to new research published in the April issue of the American Journal of Roentgenology.
Seattle consistently tops the list of regions with the lowest per capita rates of imaging utilization, while the Atlanta area leads the pack, according to researchers from Thomas Jefferson University Hospital in Philadelphia. And while low-cost procedures such as bone densitometry and mammography show little variation, over half of the imaging exams with the highest levels of variation were advanced cardiovascular studies.
Thomas Jefferson researchers used data from the U.S. Centers for Medicare and Medicaid Services (CMS) Physician Supplier Procedure Summary Master Files for 1998 to 2007 to calculate the overall procedure use rate for noninvasive diagnostic imaging procedures across 10 U.S. regions and also the ratio of the highest to lowest region for each year (AJR, April 2010, Vol. 194:4, pp. 1034 -1039). They found that over the study period, the ratio of utilization in highest and lowest regions (relative risk) ranged from 1.47 to 1.56, a more than 50% difference.
But still, this difference in utilization is more moderate than what had been previously cited in a 2008 Government Accountability Office (GAO) report on Medicare Part B spending for imaging services, which found that a nearly eightfold variation among states in Medicare imaging expenditures, from $62 in Vermont to $472 in Florida (GAO 08-452, June 13, 2008).
The GAO report examined in-office use, which skewed perceptions about the rise in geographic variation of imaging use across the U.S., according to contributing author Dr. David C. Levin.
"This [eightfold] figure came from private office utilization, but our study is concerned with overall utilization," he told AuntMinnie.com. "That number isn't useful, because maybe there are a lot more private offices in Florida, and it's as simple as that."
Use highest in Atlanta, lowest in Seattle
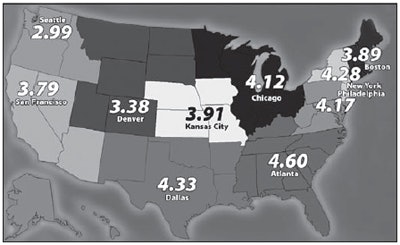
Levin and lead author Laurence Parker, Ph.D., found that in 2007, the Atlanta region had the highest utilization rate of noninvasive diagnostic imaging services, with 4.60 procedures per capita. Seattle had the lowest rate, with 2.99 procedures per capita. The relative risk (the ratio of the highest to lowest region) was 1.54.
 |
| Utilization rate per capita of noninvasive diagnostic imaging in Medicare population by Centers for Medicare and Medicaid Services geographic region in 2007. Image courtesy of the American Journal of Roentgenology (April 2010, Vol. 194:4, pp. 1034 -1039). |
Over the 10-year time frame of the study, the researchers found little change in the relative utilization rates of different regions: Except for a slight decline from 1998 to 1999, the increase is consistent and steady, about 29.3%, with a greater growth period in the middle years (pre-Deficit Reduction Act [DRA] of 2005) than at the beginning or the end of the time frame. Differences among the 10 regions were fairly consistent over the 10-year period, with the highest volumes always in the Atlanta region and the lowest always in Seattle.
The percentage change in regional noninvasive diagnostic imaging utilization rates from 1998 to 2007:
|
Variations in regional imaging use raise concerns about cost and quality, with underutilization on the low-cost, low-quality side and overutilization on the high-cost, high-quality side, Parker told AuntMinnie.com.
"If medical procedures are rationally applied, there won't be as much regional difference, except to the extent that they reflect underlying differences in illness," he said. "Substantial variations can reflect both overuse or underuse. There are so many factors that make up use rates, including access to care and access to state-of-the-art versus substandard medicine."
In 2007, the three imaging categories with the lowest regional variation, again measured by relative risk, were bone densitometry, mammography, and skeletal radiography, although six categories of advanced imaging -- CT body, CT head, CT spine, MRI head, MRI musculoskeletal, and MR spine -- also fell below the mean relative risk of 2.00 and below.
The 14 categories highest in regional variation were all advanced imaging techniques, and eight of them were cardiovascular -- a disturbing finding, Parker wrote, as cardiovascular imaging is done primarily in cardiologists' offices and is subject to self-referral issues.
Finally, 10 of these 14 categories highest in regional variation were also high-growth techniques.
"Radiology is a constantly innovating field," Parker told AuntMinnie.com. "What we inevitably see is that when a new technology is introduced, there are big growth rates in its use, influenced by a few early adopters in a region. But the rates do calm down."
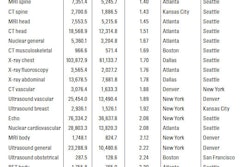
Click here to view a chart of the regional utilization rate per 100,000 beneficiary population of grouped noninvasive diagnostic imaging procedures for 2007.
Comparing 2007 utilization to 1998, the team found that overall differences between regions were lower in 1998 (relative risk of 1.49 as compared to 1.54 in 2007) and that fewer imaging categories had a relative risk greater than 2.00.
General ultrasound and breast ultrasound had lower regional variation in 1998 than in 2007 (1.72 versus 2.22 and 1.35 versus 1.92, respectively) -- another troubling finding, Parker wrote, since ultrasound is an "operator-dependent" technique, and increasing regional variations may point to variations in distribution across the country of trained staff.
Regional differences in imaging use: Here to stay?
The study required substantial "analytic compression" to compare more than 500 radiology procedures over 10 years and 10 regions, and did not explore factors such as place of service or specialty of performing physician or the effect of the DRA, Parker wrote. But the fact that regional differences in the use of noninvasive diagnostic imaging exist is clear, he told AuntMinnie.com.
"Even though we feel that the amount of variation among geographic regions in this country has been overstated, it is still substantial," he said. "And these differences aren't going away. In fact, they're getting bigger, and they need to be addressed."
By Kate Madden Yee
AuntMinnie.com staff writer
March 22, 2010
Related Reading
PET use by nonrads growing rapidly, March 2, 2010
One-quarter of outpatient CT and MR exams are inappropriate, March 1, 2010
CDC report: MRI, CT, PET use spikes in physician offices, ER, February 18, 2010
NEJM study: Imaging procedures, radiation growing, August 26, 2009
MedPAC: Self-referring docs use more imaging, June 23, 2009
Copyright © 2010 AuntMinnie.com