This article continues our series of white papers on radiologic patient positioning techniques. Appearing each month on AuntMinnie.com, the series explores each of the major modalities. If you'd like to comment on or contribute to this series, please e-mail [email protected].
Chest x-ray lateral decubitus positioning techniques
Decubitus means lying down; thus, this projection is made with the patient lying on their side and the x-ray beam horizontal (parallel) to the floor. The primary goal of performing the lateral decubitus projection is to demonstrate fluid in the pleural cavity (a pleural effusion), which is otherwise not clearly visible on a supine or upright chest radiograph.
Lateral decubitus films are helpful for determining if effusion is free-flowing, and are also used to determine whether there is enough fluid to sample by thoracentesis. A lateral decubitus projection can also be helpful in showing small amounts of air in the pleural cavity (a pneumothorax) as well as air-fluid levels in other cases.
 A case of subpulmonic effusion (pleural effusion located between the lung and the diaphragm). Subpulmonic effusions are suspected by hemidiaphragm elevation. In this case, a lateral decubitus x-ray with the patient lying on the side of the effusion is helpful not only to ensure the presence of effusion but also to quantify the volume. Image courtesy of Dr. Naveed Ahmad.
A case of subpulmonic effusion (pleural effusion located between the lung and the diaphragm). Subpulmonic effusions are suspected by hemidiaphragm elevation. In this case, a lateral decubitus x-ray with the patient lying on the side of the effusion is helpful not only to ensure the presence of effusion but also to quantify the volume. Image courtesy of Dr. Naveed Ahmad.
Patient preparation
Ask the patient to remove all clothing from the waist up, put on a hospital gown, remove any jewelry (necklace, earrings), and, if necessary, tie hair up on top of the head.
Patient position considerations
- Instruct the patient to lie on the affected side if the x-ray is being taken to determine pleural effusion -- or on the unaffected side if it is being taken to look for a pneumothorax. The side to be imaged must be determined by the requesting physician. The projection is called a right lateral decubitus if the patient is lying on the right side and a left lateral decubitus if the patient is lying on the left side.
- A lateral decubitus projection can be obtained in anteroposterior (AP) or posteroanterior (PA) view; however, the AP view is more commonly used.
- Be sure to maintain the patient in position for at least five minutes before making the exposure so that fluid in the pleural cavity can settle and air, if present, can rise.
- Place the appropriate markers to indicate which side is up (decubitus marker or arrow) on the film cassette.
Position of chest
- Instruct the patient to extend the neck, chin, and head to avoid their superimposition on the lung fields.
- The patient's arms should be extended sufficiently above the head to prevent their superimposition on the upper chest field.
- Adjust the thorax in true lateral position and make sure that the patient is not leaning forward, backward, or sideways against the grid. For an AP view, the back of the patient's chest should be placed firmly against the image receptor (IR). Ensure that there will be no rotation in the image by viewing the patient from the tube position. (Placing a radiolucent board under the patient can help reduce the possibility of rotation in the image.)
- Place a lead shield between the x-ray tube and the patient's pelvis for gonadal protection.
- When the exposure is ready to be made, ask the patient to take two deep breaths. The exposure is made at the end of the second full inspiration to ensure maximum expansion of the lungs.
Film holder placement
For lateral decubitus chest radiographs, place a 14 x 17-inch (35 x 43-cm) film holder or IR behind the patient, either crosswise or lengthwise depending on their build. Adjust the IR so that it extends approximately 1 ½ - 2 inches (4-5 cm) beyond their shoulders. The source to image distance (SID) should be at a minimum of 72 inches (180 cm).
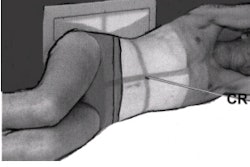
Central ray
The central ray (CR) is set horizontal and perpendicular to the center of the cassette. Using a horizontal beam is very important; otherwise air fluid levels or a pneumothorax (the primary goal of performing this projection) can be missed.
 AP projection lateral decubitus position. Image courtesy of Dr. Naveed Ahmad. Reprinted from Merrill’s Atlas of Radiographic Positions and Radiologic Procedures, 9th edition, Ballinger and Frank, page 548 (figure 10-68), copyright 1999 Mosby, with permission from Elsevier Science.
AP projection lateral decubitus position. Image courtesy of Dr. Naveed Ahmad. Reprinted from Merrill’s Atlas of Radiographic Positions and Radiologic Procedures, 9th edition, Ballinger and Frank, page 548 (figure 10-68), copyright 1999 Mosby, with permission from Elsevier Science.
For an AP projection lateral decubitus exposure, the jugular notch is used as a landmark. The CR should be directed 3-4 inches (8-10 cm) below the jugular notch that corresponds to the center of the lung fields at the T7 level (mid-thorax). For a PA projection lateral decubitus position, the CR should be directed 7-8 inches (18-20 cm) below the vertebra prominans at the level of the inferior angle of the patient's scapula.
Collimation
On each side of the posterior chest, the illuminated field margins should correspond to the outer skin margins of the patient. The upper border of the illuminated field should be above the patient's shoulders. This will result in a lower collimation border of 1-2 inches (3-5 cm) below the costophrenic angle, if the central ray was correctly centered. The collimation should be adequate to allow for some margin of error in both CR placement and lung expansion during deep inspiration.
Imaging technique
- Film size: 14 x 17 inches (35 x 43 cm)
- Exposure: 125 kVp
- mAs: 3
- cm: 21
- ML: 7
- Sk: 22
Evaluation criteria for a good lateral decubitus position (AP or PA projection)
- The entire lung field from apices to the costophrenic angles should be clearly demonstrated.
- No rotation -- the sternal ends of the clavicle should be at the same distance from the center line of the spine.
- Arms should not superimpose upper lungs.
- If the primary goal of the lateral decubitus projection is to demonstrate fluid in the pleural cavity (pleural effusion), the suspected side should be down and the affected side should be demonstrated in its entirety. Do not cut off that side of the chest in the image.
- If the primary goal of the lateral decubitus projection is to demonstrate air in the pleural cavity (pneumothorax) the suspected side should be up and the affected side should be demonstrated in its entirety.
- Appropriate markers to indicate which side is up (decubitus marker or arrow) should be placed on the film cassette.
- Sharp radiographic outline -- the outline of the diaphragm and lung markings -- should be sharp. This can be accomplished by ensuring no motion or breathing is taking place at the time of exposure.
- The vertebrae and ribs should be faintly visible through the heart shadow.
Chest x-ray oblique positioning techniques
Oblique projections are not ordered as frequently as a few years ago, because CT is more commonly employed whenever pathology is not clearly visualized on a standard chest x-ray.
However, oblique-view chest x-rays may be helpful and are requested for the following reasons:
- For separating a pulmonary or mediastinal mass or opacity from structures that overlie it on the PA and lateral views.
- For studying lesions that are visible in the PA view but not in the lateral view.
- For determining the site of origin of an intrathoracic lesion.
- Right anterior oblique (RAO) and left anterior oblique (LAO) positions are routinely used to study the esophagus in barium examinations.
- As an aid for the differential diagnosis of cardiac and great vessel enlargement.
Patient preparation
Ask the patient to remove all clothing from the waist up, put on a hospital gown, remove any jewelry (necklace, earrings), and, if necessary, tie hair up on top of the head.
Patient position
Anterior (PA) oblique projections are obtained with patient upright with respective side of the chest rotated 45 degrees against the IR. The patient's arm that is closest to the cassette should be flexed, with the hand resting on the hip. The patient's opposite arm should be raised as high as possible. The patient should be looking straight ahead, with the chin raised. Posterior oblique positions are only used when the patient is too ill to be turned to a prone position.
 Anterior (PA) oblique projections -- the side of interest is the side furthest from the cassette. Image courtesy of Dr. Naveed Ahmad.
Anterior (PA) oblique projections -- the side of interest is the side furthest from the cassette. Image courtesy of Dr. Naveed Ahmad.
Chest position
Oblique positions are named according to the chest part closest to the cassette. For anterior (PA) oblique projections the side of interest is the side furthest from the cassette.
- RAO view -- This is obtained with the right front of the patient against the cassette. The patient is turned approximately 45 degrees toward the right side, placing the patient's right shoulder in contact with the grid device and left hand on their hip. This position demonstrates the maximum area of the left lung field.
- LAO view -- This is obtained with the left front of the patient against the cassette. The patient is turned approximately 45 degrees toward the left side, placing the patient's left shoulder in contact with the grid device and right hand on their hip. This position demonstrates the maximum area of the right lung field.
- Left posterior oblique (LPO) view -- This is obtained with the right back of the patient against the cassette. The patient is rotated 45 degrees with left posterior shoulder against the IR. It is comparable to an RAO view in demonstrating the maximum area of the left lung field.
- Right posterior oblique (RPO) view -- This is obtained with the left front of the patient against the cassette. The patient is rotated 45 degrees with right posterior shoulder against the IR. This position is comparable to an LAO view demonstrating the maximum area of the right lung field.
Place a lead shield between the x-ray tube and the patient's pelvis for gonadal protection. When the exposure is ready to be made, ask the patient to take two deep breaths. The exposure is made at the end of the second full inspiration to ensure maximum expansion of the lungs.
Central ray
The CR should be perpendicular to the center of the cassette at the level of T7.
Film holder placement
The cassette or IR should be 14 x 17 inches (35 x 43 cm) lengthwise. The SID should be at a minimum of 72 inches (180 cm).
 A right anterior oblique (right image) and left anterior oblique (left image) view demonstrate maximum area of the lung field. Image courtesy of Dr. Naveed Ahmad.
A right anterior oblique (right image) and left anterior oblique (left image) view demonstrate maximum area of the lung field. Image courtesy of Dr. Naveed Ahmad.
Evaluation criteria for a good oblique chest projection
- Both lungs, from the apices to the costophrenic angles, should be included.
- The maximum area of the right lung field should be demonstrated on an LAO and RPO view.
- The maximum area of the left lung field should be demonstrated on an RAO and LPO view.
- The distance from the outer margin of the ribs to the vertebral column on the side furthest from the IR should be approximately two times the distance of the side closest to the IR. This is to evaluate 45-degree rotation.
- The diaphragm and heart borders should be sharp with no motion.
- On an AP oblique projection, the heart and great vessels appear magnified.
AuntMinnie.com contributing writer
December 21, 2001
Copyright © 2001 AuntMinnie.com