Detection rather than characterization is the main stumbling block for radiologists who are learning to interpret virtual colonoscopy (VC) exams, according to a study out of the Mayo Clinic in Rochester, MN. Dr. Jeff Fidler presented the results of a survey conducted at his institution last week at the American Roentgen Ray Society meeting in San Diego.
"As CT colonography becomes more popular, there is an increasing demand for radiologist education," Fidler said. While there are ways for radiologists to learn more about virtual colonoscopy through site visits or published articles, there is limited data on the case mix that radiologist would see in a virtual colonoscopy program, he said.
For this study, 15 radiologists who were seeking to acquire or improve their VC reading skills completed a questionnaire after utilizing an interactive, tutorial program. While all of the readers were experienced in abdominal imaging, they had no or little experience with virtual colonoscopy, Fidler said.
The virtual colonoscopy electronic tutor developed by Fidler’s co-author, Dr. Joel Fletcher, consisted of two parts:
- Limited datasets that demonstrated the varied appearances of polyps, cancers, and pitfalls in interpreting exams.
- A 50-question test of complete datasets (supine and prone images) and made up for 20 normal exams; 26 polyps (size range of 0.5-5.0 cm), 8 cancers, and 1 lipoma.
Polyp morphologies included 15 sessile, 6 pedunculated, and 5 flat lesions. The cancer morphologies were 2 flat infiltrating lesions, 3 polypoid lesions, and 3 annular constricting lesions.
After reviewing each case, the radiologist was asked to indicate if and where a polyp was visualized. The tutorial program then showed each lesion to the radiologist and, if the lesion went undetected, the reader stated on the questionnaire if the lesion was simply not seem; was seen but interpreted as normal wall or fold; or was seen but interpreted as stool or fluid.
According to the results, the sensitivities for the detection of polyps of all sizes ranged from 38%-81% (mean 66%). The majority of errors, 55%, were failures of detection while 45% were errors in characterization. Of the 56 characterization errors, the readers identified polyps as normal folds or walls in 41 cases, and intraluminal material in 15 cases.
"Flat polyps were most frequently missed, followed by pedunculated polyps," Fidler said. Five reviewers missed 1 cancer each while 3 reviewers missed 2. All of the missed cancers with the exception of 3 were secondary to failure in detection. The most frequently missed cancer was an annular constricting tumor.
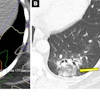
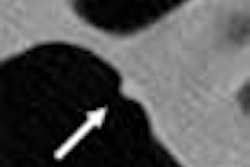
Fidler offered some examples of commonly missed flat polyps, including a 2-cm flat adenoma on the fold, and a 1.5-cm adenoma in the cecum. Among the pedunculated polyps, the readers missed a 1-cm adenoma in the sigmoid. Among the cancers, a 3.3-cm flat cancer in the splenic flexure on the fold was commonly missed.
"Examples of these abnormal cases should be emphasized in CTC training programs," Fidler concluded.
Session attendee Dr. Michael Zalis from Massachusetts General Hospital in Boston asked Fidler if his group had done any follow-up studies on the radiologists to see if their skills had improved over time. Fidler said they had not done any follow-up, although it would be limited to the four radiologists on staff at the Mayo Clinic. The remaining participants were visiting physicians at the time the survey was conducted, he said.
In a subsequent paper, Fidler reported that the addition of computer-aided detection to CTC reading did improve results to some degree. Out of 20 polyps, the CAD program detected 40% of all polyps greater than 1 cm, and 43% of all adenocarcinomas greater than 1 cm in size. However, CAD did not find any flat polyps beyond what was spotted by two interpreting radiologists.
By Shalmali PalAuntMinnie.com staff writer
May 13, 2003
Related Reading
Multislice CT may improve virtual colonoscopy results, May 2, 2003
Colon CAD finds complementary role with radiologists, April 23, 2003
Virtual colonoscopy aces first flat-lesion study, December 3, 2003
Copyright © 2003 AuntMinnie.com