Virtual colonoscopy providers have been known to get excited about novel viewing systems on the horizon, and for good reason. New techniques such as colon dissection and Mercator projections could potentially supplant the most common interpretation approach, e.g., axial viewing combined with 3-D for problem-solving of virtual colonoscopy studies.
Clinical studies are few and far between, however, which makes recent research by Dr. Hanno Hoppe and colleagues from Inselspital University Hospital in Bern, Switzerland, all the more interesting. Hoppe's group fired up the virtual colon dissection (VCD) software in the CT colonography package of their GE Advantage Workstation (GE Medical Systems, Waukesha, WI) and compared the technique with axial viewing plus 3-D problem-solving, as well as with conventional colonoscopy.
"Virtual colonic dissection is a new visualization mode for CT colonography," Hoppe said in a presentation at the 2003 European Congress of Radiology in Vienna. "There exist various viewing modes for CTC, and the question is which one is best to use for analysis. A complete 3-D fly-through of the colon is quite tedious and time-consuming. Viewing axial slices with 3-D for problem-solving is preferred by most readers at the moment. However, a new viewing mode, colonic dissection, has recently become commercially available and needs to be evaluated."
In the study, 20 patients with suspected colonic polyps or cancer had standard bowel preparation before undergoing virtual and conventional colonoscopy on the same day. Virtual colonoscopy data were acquired in both prone and supine positions using a four-row multidetector CT scanner with collimation set at 4 x 2 mm and a reconstruction interval of 1 mm, Hoppe said. Axial and dissection views of the data were read independently in two viewing sessions by two radiologists blinded to the results.
"If a polyp was suspected it was confirmed with additional 2-D and 3-D views," he said. "The analysis time was recorded for both methods, and, especially for virtual colon dissection, the number of reconstructed colonic segments and the number of software failures that occurred was recorded."
 |
| Virtual colonic dissection (VCD) shows a 5-mm sessile rectal polyp (arrow). VCD creates a 3-D panel of the inner colonic surface. The left upper corner represents the most aboral and the right lower corner the most oral portion of the colon. Image courtesy of Dr. Hanno Hoppe. |
The VCD software package opens up and unfolds the colon virtually, and visualizes its internal surface in three dimensions, Hoppe said. "For use of virtual colon dissection, first a central colonic path needs to be defined within the colon dataset. Second, the virtual colon is unfolded along this longitudinal axis, and so the surface of the colon is visualized in 3-D. Once the center part of the colon is defined, the software generates a panel of the inner view of the colonic surface.... This panel has a field of view of 90° , and in order to view the entire mucosal surface, you can shift the field of view in increments of 45° ."
According to the results, conventional colonoscopy found 25 polyps (≤ 5 mm: n=12, 6-9 mm: n=8, ≥ 10 mm: n=5).
 |
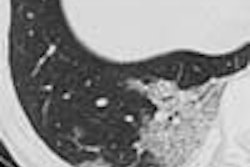
| The same 5-mm sessile rectal polyp is clearly depicted in the 2-D axial view (left) and in the 3-D endoscopic view (right). Images courtesy of Dr. Hanno Hoppe. |
Virtual colon dissection (VCD) achieved 78% sensitivity for the detection of lesions 10 mm and larger, compared with 95% for axial viewing with 3-D problem-solving. For all lesions smaller than 10 mm, sensitivity was 50% for VCD and 42% for axial reading with 3-D problem-solving.
 |
| Chart above shows lower overall sensitivity for virtual colon dissection viewing compared with the commonest virtual colonoscopy approach: axial plus 3-D for problem-solving. Data courtesy of Dr. Hanno Hoppe. |
Analysis was slower with VCD as well, with a mean of 37.2 minutes (range 22 min-60 min) per patient compared with 29 minutes for axial viewing with 3-D problem-solving, Hoppe said. And VCD achieved successful visualization of the entire prone and supine datasets in just 35% of patients, part of the data in 45% of patients, and no data in 20% of patients. Hoppe said the software failed six times in all, and that the VCD images were somewhat small for optimal viewing.
The VCD image quality was "superb," he said. "And at the moment the overall detection rate is not superior in axial reading. But because the software has a high failure rate, it tends to be more time-consuming than axial readings. So although the software seems to be very promising, improvement is needed."
By Eric BarnesAuntMinnie.com staff writer
July 9, 2003
Related Reading
No size, grade correlation seen in enhancement of colorectal cancer, June 9, 2003
Electronic virtual colonoscopy tutor emphasizes spectrum of abnormalities, May 13, 2003
Multislice CT may improve virtual colonoscopy results, May 2, 2003
Colon CAD finds complementary role with radiologists, April 23, 2003
Copyright © 2003 AuntMinnie.com