Innovative display techniques are an important part of the high-tech future that virtual colonoscopy providers are eyeing hopefully. The interest in new solutions stems from shortcomings in existing interpretation techniques, which are adequate but far from ideal.
Two-dimensional slice review, currently the predominant approach to virtual colonoscopy, requires radiologists to sift through mountains of CT data that bear little resemblance to colonic mucosa. The need to problem-solve equivocal findings with multiplanar reconstructions or 3-D endoluminal views is routine.
Primary 3-D interpretation has its own issues, requiring frequent reference to 2-D slices for problem-solving, and raising questions about how much of the mucosal surface is actually examined, and in how much time.
"Findings in several studies, however, suggest that the primary use of 3-D views results in higher sensitivity," wrote Frans Vos, Ph.D., Rogier van Gelder, and colleagues in the September issue of Radiology. "Beaulieu et al demonstrate a significantly better outcome with 3-D modes after correction for lesion visibility" (Vos et al, Radiology, September 2003, Vol. 228:3, pp. 878-885; Beaulieu et al, Radiology, July 1999, Vol. 212:1, pp. 203-212).
A number of bolder solutions have been investigated as well, such as the Mercator projections of Paik et al, or mathematical flattening schemes, added Vos and colleagues from the Academic Medical Center in Amsterdam. But many of these techniques present problems relating to severe distortion of the mucosal surface, such as the appearance of abnormalities in more than one area.
In the latest article, the Dutch researchers compared conventional 3-D interpretation with a new cubed display technique. The new system speeded up interpretation time significantly, while increasing the percentage of the mucosal surface examined.
"To overcome the current limitations of 3-D imaging, we developed an alternative 3-D display method that renders six planar projections (unfolded cube display) at 90° viewing angles from points on the central path," they wrote. "The unfolding of such a cube shows the complete field of view at a path position. The aim of the images sequence of unfolded cubes is to facilitate rapid exploration of the entire colon wall."
The study examined 30 patients (13 men, 17 women) at increased risk for colorectal cancer. Fifty-four percent had had polyps previously; the rest had a family history of colorectal cancer. All patients underwent same-day virtual and conventional colonoscopy.
A day before the CT exam, the patients underwent standard bowel cleansing by drinking 4-6 L of macrogol solution (KleanPrep, Helsinn Birex Pharmaceuticals, Dublin, Ireland), in addition to intravenously administered butyl scopalamine (Buscopan; Boehringer Ingelheim, Ingelheim, Germany) to reduce peristalsis. Manual colon insufflation with a mixture of CO2 and room air was used in all of the subjects.
Multislice CT images were acquired on an Mx8000 scanner (Philips Medical Systems, Andover, MA) in both prone and supine positions, using scan parameters of 120 kVp, 167 mAs, collimation of 4 x 2.5 mm, pitch 1.25, and a standard reconstruction filter. The effective section thickness was 3.2 mm with an overlap of 1.6 mm, according to the authors.
Three-dimensional technique
In the conventional 3-D display method, antegrade and retrograde cine loops were evaluated on a Philips EasyVision workstation, with images volume-rendered at positions 4 mm apart along the central colon lumen. Voxel values less than -650 HU were rendered as zero, and therefore transparent. The viewing angle was set to 120° to compromise between image distortion and surface visibility, and the volume-rendering transfer function, sampling, and frame rate were equal to those used in the unfolded cube display.
Cube technique
"To avoid extreme deformations while showing the full visible field around a position, we introduced a series of unfolded cube renderings," Vos and colleagues wrote. "The unfolded cubes were also generated by means of sampling on the central path through the colon. A cube was virtually placed on each such point, and on the cube faces, 90° views from the center were projected.... Real-time rendering of the corresponding wall part also facilitated local inspection of the surface by means of adaptation of the virtual camera position and orientation."
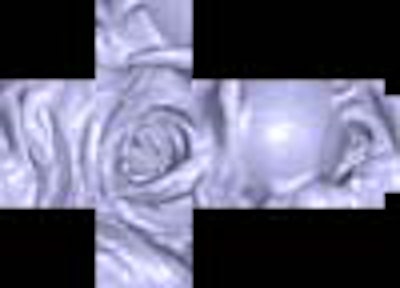
 |
| Typical example of a polyp in conventional 3-D display (above) and in unfolded cube display (below). Images copyright © RSNA 2003, republished with permission of the Radiological Society of North America and the authors, from Radiology, September 2003, Vol. 228:3, pp. 878-885. |
 |
An abdominal radiologist and research fellow, both experienced in virtual colonoscopy exams, reviewed the data with both systems, while remaining blinded to the conventional colonoscopy results. The outcomes were analyzed to measure evaluation time and stratified according to the presence of polyps, and surface visibility was gauged as the percentage of colon surface voxels coming into view.
According to the results, mean evaluation time with conventional 3-D was 36 minutes, 49 seconds with observer 1, and 35 minutes, 5 seconds with observer 2, significantly slower than with the unfolded cube display (19 minutes 33 seconds for observer 1, 20 minutes 9 seconds for observer 2). The differences between observers were not statistically significant, and the presence of polyps did not significantly increase interpretation times, the group added.
With the conventional 3-D display, antegrade and retrograde views resulted in 93.8% visibility of the colonic mucosa, compared to 99.5% using the unfolded cube display, a significant difference (P<0.05)
 |
| Left, unfolded cube display. Right, conventional 3-D display. Areas in black were missed. Images copyright © RSNA 2003, republished with permission of the Radiological Society of North America and the authors, from Radiology, September 2003, Vol. 228:3, pp. 878-885. |
No significant differences in sensitivity and specificity and were seen between the two methods, they wrote. Interobserver agreement was high as well: k=0.692 for the unfolded cube display, and k=0.605 for the conventional 3-D display.
Per-patient sensitivity for large and medium polyps was not significantly different between the two methods, the authors wrote. With conventional colonoscopy as a reference standard, observer 1 found 8 of 8 polyps using both displays; observer 2 found 7 of 8 with the conventional display and all 8 with the cubed display. The conventional display did reduce sensitivity for the detection of small polyps for observer 1 (16/69, compared with 27/69 using the cubed display), but the choice of display method for smaller polyps did not significantly affect sensitivity in observer 2 (conventional 3-D 26/69, unfolded cube 24/69).
"Several methods have been explored for optimization of the amount of colon surface coming into view," the authors wrote. "The viewing angle may be increased, but this is at the expense of severe deformation toward the edges of the image. A so-called flattening method can be used to straighten the colon mathematically. Thus, images of large surface areas of the colon are generated that are similar to gross pathology specimens. Unfortunately, such an approach may yield severe distortion, which causes lesions to appear more than once in different areas."
Mercator and stereography projections were compared by Paik et al, who concluded that Mercator projections distinguished true-positive findings from the environment better than stereographic or panoramic views, the authors continued. "A generally recognized drawback of Mercator projection, however, is that the image becomes distorted away from the equatorial region," they wrote. "Such image deformation would restrict the sensitivity in areas where the colon is strongly curved" (Journal of Computer Assisted Tomography, March-April 2000, Vol 24:2, pp. 179-188).
"The (unfolded cube) method is more time-efficient and yields better surface visibility than does a conventional 3-D technique," the authors concluded.
By Eric BarnesAuntMinnie.com staff writer
October 6, 2003
Copyright © 2003 AuntMinnie.com
















![Images show the pectoralis muscles of a healthy male individual who never smoked (age, 66 years; height, 178 cm; body mass index [BMI, calculated as weight in kilograms divided by height in meters squared], 28.4; number of cigarette pack-years, 0; forced expiratory volume in 1 second [FEV1], 97.6% predicted; FEV1: forced vital capacity [FVC] ratio, 0.71; pectoralis muscle area [PMA], 59.4 cm2; pectoralis muscle volume [PMV], 764 cm3) and a male individual with a smoking history and chronic obstructive pulmonary disorder (COPD) (age, 66 years; height, 178 cm; BMI, 27.5; number of cigarette pack-years, 43.2, FEV1, 48% predicted; FEV1:FVC, 0.56; PMA, 35 cm2; PMV, 480.8 cm3) from the Canadian Cohort Obstructive Lung Disease (i.e., CanCOLD) study. The CT image is shown in the axial plane. The PMV is automatically extracted using the developed deep learning model and overlayed onto the lungs for visual clarity.](https://img.auntminnie.com/mindful/smg/workspaces/default/uploads/2026/03/genkin.25LqljVF0y.jpg?auto=format%2Ccompress&crop=focalpoint&dpr=2&fit=crop&h=167&q=70&w=250)
