The distinctions among tumor types have become more important with the rapid evolution of CT image quality. The vendors' latest prototype scanners go even smaller and all of the vendors are headed toward isotropic imaging. What was once an indeterminate finding can now be seen in great detail.
With multidetector-row CT scanners picking up smaller and smaller lung abnormalities, thoracic radiologists are playing a kind of catch-up with the technology. In other words, they're looking for new algorithms to examine, follow up, and treat more lung cancers while they're curable.
"We're starting to think about smaller lung cancers," said Dr. David Yankelevitz in a talk at the 2003 Multidetector Row CT symposium in San Francisco. "How do we work these up? ...We've introduced this terminology: solid, part-solid and non-solid, according to the extent to which the parenchyma within the nodules is completely obscured. I prefer this terminology because I like to think of nodules as what they are. I don't like to think of them as opacities, I don't think of them as attenuations. When we look at blood vessels we don't call them tubular opacities, we call them blood vessels."
The differences go beyond semantics -- the findings speak volumes about the prognostic implications of the abnormalities, Yankelevitz said. Part-solid nodules in particular have a very high frequency of malignancy, he said, even more than do solid or non-solid lesions.
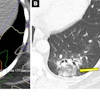
"These part-solid nodules can have linear extensions extending from them, in fact, very consistently. Pathologically they've been shown to correlate with extension of the lymphatic system," he said. "And you can also see this pattern (in) dilated bronchi within these part-solid lesions. It's interesting when you biopsy these, you often get fibrotic material that comes out; you have to be very careful. These tend to be in areas of fibrosis that perhaps causes the dilatation of these bronchi."
 |
| Part-solid nodule with linear extensions. All images courtesy of Dr. David Yankelevitz. |
Japanese researchers have found distinct prognostic differences among nodule types in thin-section CT, Yankelevitz said. In a Radiology study, for example, Aoki and colleagues found that adenocarcinomas smaller than 2 cm with a ground-glass component of more than 50% were highly unlikely to have lymph node metastases or vessel invasion. The group concluded that thin-section CT may be a helpful tool in determining the eligibility of patients for resection (Radiology, Sept. 2001, Vol. 220:3, pp. 803-809).
 |
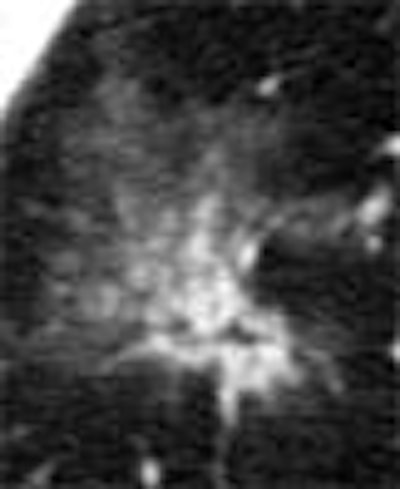
| Non-solid nodule. |
The distinctions among tumor types have become more important with the rapid evolution of CT image quality. Yankelevitz recalled that when he first began doing CT chest scans in 1993, imaging in a single breathhold meant using a minimum 10-mm slice thickness. As scanner technology improved, the minimum slice thickness dropped to 5 mm, then 2.5 mm, then 1 mm. The vendors' latest prototype scanners go even smaller, he said, and all of the vendors are headed toward isotropic imaging. What was once an indeterminate finding can now be seen in great detail.
 |
| Non-solid nodule at baseline (left) and follow-up (right). |
"So the future is very bright," he said. "And if you combine (thinner slices) with the image processing that's currently being developed, I think there's going to be a dramatic improvement in what we can detect."
None of which has made nodule assessment an easy job. CT lung scans are still complicated by motion artifacts, for example, and by differences in inspiration and positioning between one study and the next. Some nodules have blood vessels attached, or are obscured by adjacent structures.
For example, a nodule should generally be biopsied if its attenuation is 15 HU or higher following contrast administration, Yankelevitz said. But the rule doesn't work well when nodules are smaller than 1 cm.
 |
| Non-solid nodule pre- and post-contrast. |
One screening algorithm doesn't fit all
With nodules appearing in any number of patterns and types and circumstances, no single workup or follow-up protocol is appropriate for all of them. Finally, lesion work must be undertaken in the context of the individual patient, Yankelevitz said.
This means that while screening algorithms can be standardized in a large study population with similar characteristics, the approach must be individualized for the patient who walks in the door on his own. And the choice of algorithm makes an enormous difference in the effectiveness of the imaging program, he said.
Nodule assessment
A number of general considerations apply when examining lung abnormalities with CT, Yankelevitz said.
There is the spiculated shape suggestive of malignancy, for example, and the classic benign pattern of a calcified nodule that has not changed in 2 years; these aren't new. The problem with the models is that they were developed for diagnosing the larger nodules detected by older scanners, he said; they are not always applicable to today's world of subcentimeter abnormalities.
 |
| Non-solid nodule. |
"Calcification is wonderful (as a sign of benignity) when you see it, but you don't see the smaller lesions with ring patterns of calcification," Yankelevitz said. "...So it's really a whole new ballgame that we're in. I can tell you I've seen many hamartomas that are subcentimeter. I haven't seen a single one that has fat in it. So you don't see fat in hamartomas, at least in my experience. You don't see the calcifications in popcorn patterns in hamartomas. So I think we have to get to better and better criteria for this smaller subcategory (of nodules).
Likewise, although nodules are suspect if their attenuation is 15 HU or higher following contrast administration, the smallest nodules don't always enhance significantly, he said.
Once the potentially troublesome nodule is detected, it can be diagnosed with minimal invasiveness by bronchoscopy or transthoracic needle biopsy, or more invasively by thoracoscopy or thoracotomy. But all methods aren't created equal. Yankelevitz said he has a hard time seeing any role for bronchoscopy in diagnosing smaller nodules, though the technique is certain to improve.
"The needle biopsy is just much better," he said. "In terms of invasive (techniques), diagnosing a lesion with thoracotomy is not the way. I mean, sure there are going to be cases where you have to do something more invasive surgically, but it's got to be thoracoscopy. I just don't see a role for doing thoracotomy. I think we're well beyond that aspect of diagnosis."
PET for staging, not yet for screening
Overall, FDG-PET imaging has demonstrated overall sensitivities of 83%-97%, and specificities of 63%-90% for the detection of lung malignancy. But its accuracy depends on lesion size, and the technique fares poorly for the detection of subcentimeter lesions, Yankelevitz said.
"But I think right now PET has a tremendous role in staging," he said. One study showed that up to 18% of patients considered resectable are deemed unresectable after PET scanning. PET has been shown to alter nodal CT staging as often as 24% of the time. And it is well known for its ability to detect extrathoracic metastases.
A study in this month's Radiology showed that PET/CT significantly improved the staging of non small-cell lung cancer compared to either modality alone. Compared to PET data, PET/CT led to a change in tumor stage in 7/27 (26%) of NSCLC patients. And compared to CT data alone, PET/CT staging was 30% more accurate (Radiology, November 2003, Vol. 229:2, pp. 526-533).
New radiotracers such as C-choline, and combined PET/CT imaging are two developments that could move PET ahead in the future, Yankelevitz said.
Calculating nodule growth rates
Follow-up CT offers great potential for measuring the growth of lung abnormalities, he said, especially with the aid of imaging techniques such as volumetric analysis. In a study published this month, Yankelevitz and colleagues conclude that the follow-up interval needed to accurately assess nodule growth is inversely proportional to the nodule size at baseline.
"Less than 5-mm nodules, it takes approximately six months, at least, before you can reliably show growth," he said. "Between 5 and 10 mm (in size, the minimum interval is) somewhere between 3 and 4 months, taking into account all the variations in scanning, etc. And I think this will be quite helpful in terms of designing algorithms." (IEEE Transactions on Medical Imaging, October 2003, Vol. 22:10, pp. 1259-1274).
"And you can evaluate the growth rates in different parts; the solid and non-solid components (of the nodule) can be evaluated separately," he said. "So different aspects of this, different protocols, different workups, amounts of time between scans, it's going to be different for the different subtexts of abnormalities that we find."
 |
| Volumetric analysis of nodule size shows a doubling rate of greater than 750 days. |
Biopsy technique
Fine-needle aspiration is highly size-dependent and operator-dependent, he said, and the most important consideration for biopsying small nodules is the ability to adjust the needle. When the aim is off, the radiologist can withdraw the needle a little bit and give it another try without repuncturing the pleura. Pulmonary hamartomas tend to roll off the needle, he said, and can be quite challenging to puncture.
"Onsite cytology makes an enormous difference -- to have somebody there telling you whether you have an adequate sample or not," he said. "And there are certainly complications that can occur."
By Eric BarnesAuntMinnie.com staff writer
November 14, 2003
Copyright © 2003 AuntMinnie.com