
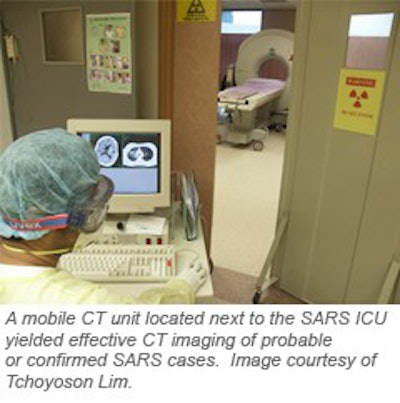
A mobile CT system can aid in providing effective radiology service to SARS patients while maintaining appropriate isolation procedures, according to researchers from the National Neuroscience Institute and Tan Tock Seng Hospital in Singapore.
"Isolation is an important key (to controlling infection)," said Dr. Hemant Parmar. "In this respect, a mobile CT scanner proved to be an invaluable alternative to the fixed CT scanner. This ensured that our department remained free from infection, and we could continue providing radiology service to the non-SARS group of patients."
Parmar discussed his institution’s radiology experience during the SARS outbreak in a scientific session at the 2003 RSNA meeting in Chicago. The researchers also published an article in the American Journal of Roentgenology(January 2004, Vol. 182:1, pp. 57-60.)
During the SARS outbreak in March and April 2003, hospital inpatients were divided into two categories: confirmed/probable SARS and non-SARS. In the interest of isolating the main radiology department, the unit was closed to SARS cases, although it continued to provide radiology service to non-SARS patients, Parmar said.
To handle the imaging needs of SARS patients, the institution decided to take a mobile CT scanner (Tomoscan M, Philips Medical Systems, Andover, MA) that was being used by the neuroradiology service and repurpose it for SARS imaging in an isolation intensive care ward. To house the system, a room that was originally a four-bed cubicle was equipped with oxygen and vacuum suction equipment, as well as other necessary life support systems.
The system was outfitted with a portable power injector (Mark IV, Medrad, Indianola, PA), and 10 1.5-mm Pb-equivalent portable lead shields for radiation protection (S&S X-Ray Products, Houston). Strict barrier nursing was carried out during all scans, and radiographers (who were assigned exclusively to the mobile CT unit) in direct contact during patient positioning wore N95 masks, gowns, gloves, and goggles, according to the researchers.
Disposable plastic covers were used on control surfaces of the scanner console during each study. After each patient left, the scanner gantry and bed were disinfected with sodium dichloroisocyanurate (5,000 ppm), Parmar said.
 |
The studies were then routed over the hospital's local-area network to the PACS (PathSpeed 8.12, GE Medical Systems, Waukesha, WI), and read remotely in the main department via PACS workstations. In the first five weeks of service, Tan Tock Seng Hospital performed 90 mobile CT studies, including 30 head, 34 thorax, and 26 abdomen/pelvis exams.
All patients tolerated the studies without incident, and there were no failed studies due to patient movement, Parmar said. There were no suspected or reported cases of patients developing SARS after being examined on the mobile scanner. Images and reports were also available on SARS ward computers via a Web browser, minimizing physical contact.
The PACS network allows for on-demand, digital viewing that was "sterile," co-author Tchoyoson Lim told AuntMinnie.com in an e-mail. No cases of infection of healthcare workers were reported.
"Although I don’t think anybody got infected with the SARS virus as a result of film contact, it was, as you could have imagined at the time, a confidence boost to the staff that movement and contact could be kept to a minimum," he said.
When it was first proposed that the mobile CT unit be used for this application, there were concerns initially that it might not have the capacity to produce acceptable images, especially for pulmonary embolism assessment, Lim said. In the 18 studies performed for that application, technical problems were indeed encountered as patients had trouble holding their breath during the slightly longer scanning time, the researchers said.
"However, the quality of images was adequate for us to confidently exclude embolism at the segmental branches of the pulmonary artery," the researchers wrote in AJR.
The mobile CT system does suffer from technical disadvantages compared with state-of-the-art multidetector CT scanners, including lower tube heat-loading capacity and longer scan time, Parmar said. In addition, breathholding is difficult for chest scans, and the images offer suboptimal resolution for some applications.
"We were not able to see the smaller divisions of the pulmonary vasculature, nor were we able to perform multiphasic studies for the abdomen," he said.
Referring clinicians provided overwhelmingly positive feedback, however, and the system proved to be a reliable alternative to a fixed CT system, Parmar said. The SARS outbreak also reinforced the need to have a strong radiology team in place, according to Lim.
"After our volunteer SARS (mobile CT) team stepped up to the plate and did their job, we know we have a good team," Lim said. "So appreciate and protect the radiology staff: they are too precious to lose."
By Erik L. RidleyAuntMinnie.com staff writer
January 22, 2004
Related Reading
The Asian-Oceanian Textbook of Radiology, January 13, 2004
WHO chief bracing for new SARS outbreak, October 9, 2003
WHO warns of resurgence of SARS, other diseases, September 8, 2003
Thin-slice CT reveals severe lung abnormalities in SARS patients, July 7, 2003
Chest CT useful in diagnosing questionable SARS cases, May 19, 2003
Copyright © 2004 AuntMinnie.com


















