The American Thoracic Society (ATS) has updated its recommendations for diagnosing and managing nonmalignant disease induced by asbestos exposure. The guidelines, first published in 1986, make the case for incorporating CT exams as an official component of asbestos-related imaging.
"Nonmalignant asbestos-related disease refers to the following conditions: asbestosis, pleural thickening or asbestos-related pleural fibrosis, 'benign' pleural effusion, and airflow obstruction," wrote the ATS subcommittee that prepared the statement in the latest issue of the American Journal of Respiratory and Critical Care Medicine. The subcommittee was chaired by Dr. Tee Guidotti from George Washington University Medical Center in Washington, DC.
Despite a ban on asbestos use in most Western countries, the volatile fiber bundles still pose a danger to 1.3 million construction workers in the U.S. However, while "there is a strong statistical association between asbestos-related disease and malignancy," the group wrote, "the majority of patients with nonmalignant asbestos-related disease do not develop cancer" (AJRCCM, September 15, 2004, Vol. 170:6, pp. 691-715).
The 24-page document offers criteria for diagnosis, suggestions on how to satisfy these criteria, descriptions of the clinical implications for diagnosis, and a basic management plan.
With regard to imaging, the authors state that chest radiographs are still an "extremely useful" tool for asbestos-related imaging, but they acknowledge that x-rays are limited in sensitivity and specificity in the early stages of asbestosis and mild pleural disease.
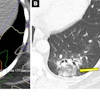
They also noted that "conventions for classifying digitized films and other advanced imaging systems have lagged behind the development of the technology." They praised conventional CT as superior to chest films for identifying parenchymal lesions, rounded atelectasis, and pleural plaques.
They also recommend high-resolution CT (HRCT) for cases in which the x-ray findings are equivocal or difficult to interpret because of the modality's limitations.
"HRCT is more specific than plain chest radiographs, excluding such conditions as emphysema, vessel prominence, overlying pleural disease, and bronchiectasis, which may confound radiographic interpretation," the group wrote.
The statement also includes the following imaging recommendations:
- HRCT scans done at 2-cm intervals can detect early pleural thickenings, evidence of fibrosis in asbestosis, and honeycombing in advance of disease.
- Radiographic evidence of pleural disease may include pleural thickening and plaques, although other abnormalities may mimic the latter on x-ray. Axial CT may fail to show diaphragmatic plaques.
- Rounded atelectasis, or folded lung, presents radiographically as a mass and as a classic "comet sign" on HRCT.
- For the assessment of chronic airway obstruction, airflow abnormalities may be associated with emphysema on x-ray. Diffusive pleural thickening and active inflammation on HRCT have been associated with worsening obstruction.
Other nonimaging tests that should be considered are bronchoalveolar lavage and pulmonary function tests, such as spirometry, lung volume tests, and carbon monoxide diffusion capacity exams, the authors wrote.
The report also stressed the importance of taking a comprehensive occupational and environmental history of patients, as well as implementing a thorough management plan. Many "modern" cases of nonmalignant disease (post-World War II) are in workers who have been exposed to asbestos for a shorter period of time, but who may progress to more advanced disease stages, due in part to a longer lifespan, the authors cautioned.
By Shalmali Pal
AuntMinnie.com staff writer
September 15, 2004
Related Reading
Part I: The back story on asbestos x-ray B readers, September 7, 2004
Part II: A survey of asbestos-related imaging, September 7, 2004
Study sounds alarm over integrity of expert readers' testimony, August 6, 2004
Separating inflammation from malignancy on thoracic FDG-PET, April 9, 2004
Asbestos-related cancer on the rise in UK, February 2, 2004
Copyright © 2004 AuntMinnie.com