European researchers have been known to take low-dose CT exams to new levels of low, but a new study from Germany tests even continental norms. What's more, the method seems to work. When Dr. Valentina Romano and colleagues at Berlin's Charité Hospital cranked their thoracic CT exam down to the level of a two-view chest x-ray, they found the technique performed nearly as well as a standard CT exam in detecting pulmonary nodules.
Dose reductions exceeding 90% are feasible in thoracic CT exams, Romano said in a November 28 presentation at the RSNA meeting in Chicago. Romano, along with Drs. Uta Zaspel, Patrick Hein, Patrick Rogalla, and others examined 106 patients (ages 23-89, 48% women, 52% men) with thoracic multidetector-row CT to rule out pulmonary nodules. The indications included staging or restaging patients with extrathoracic malignancy or primary lung cancer, or suspected pulmonary nodule on chest x-ray.
"In order to keep the total radiation dose at the level of a (two-view) chest x-ray, we replaced the scout view with a nonenhanced ultra-low-dose CT technique," Romano said. As a result, each patient was scanned twice on a 16-slice Aquilion scanner (Toshiba Medical Systems, Tokyo). First with the ultra-low dose technique: 3.5 effective mAs, 120 kVp, 16 x 1 mm collimation, pitch 1.43; then with a standard-dose protocol set at 52.2 effective mAs, but otherwise unchanged. Dose modulation was not used, and all patients underwent precisely the same imaging protocol regardless of body habitus, for which data was not collected, Romano said.
Two experienced radiologists reviewed the axial images by consensus -- first the ultra-low-dose images, followed immediately by the standard-dose images for the same patient. The radiologists assessed the number, size, location, morphology, and characterization of each nodule detected, as well as whether it appeared to be benign or malignant.
When more than five nodules were detected, the results were categorized as "many" (6-20 nodules), "multiple" (21-50 nodules), or "diffuse" (> 50 nodules), and maximum and minimum diameter was determined for each finding. Subjective diagnostic confidence in detection, characterization, and artifacts were evaluated on a scale from 1 (min) to 10 (max) for each of the two protocols.
"We basically evaluated axial images," Romano told AuntMinnie.com. "Coronal, sagittal, and thin slices for purposes of reconstruction (MPRs) were available at all times."
The readers were asked to state whether the ultra-low-dose technique had hindered either the detection or characterization of nodules.
 |
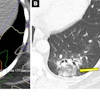
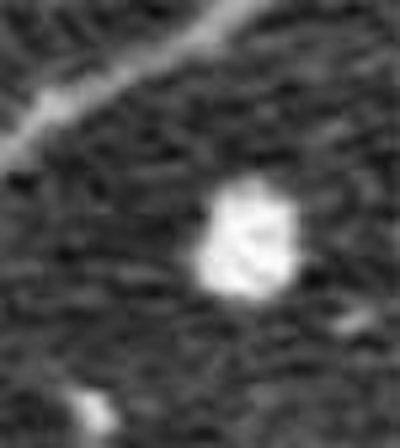
| Axial images show pulmonary nodule in standard dose (right) and ultra-low-dose scan protocols in a 64-year-old patient with prostate cancer. The zoomed images show one of two metastases that were histologically confirmed and resected. All images courtesy of Dr. Valentina Romano. |
"There was moderate agreement in the readers' subjective confidence in pulmonary nodule detection between the two methods, (k = 0.437, p < 0.05)," Romano said, adding that the readers considered the low-dose method a hindrance for nodule characterization in 10.4% of nodules (k = 0.558, p < 0.04), with misses in the ultra-low-dose technique confined to the very smallest nodules. Edges were sometimes harder to define in the lowest-dose images, which could potentially raise questions about their morphology. Still, no nodule 2 mm or smaller was overcounted in the low-dose technique, while 16.1% were undercounted, she said.
 |
| Coronal view of ultra-low-dose protocol reveals a solitary nodule in a 36-year-old patient with monolateral breast cancer (no histologic assessment was available). |
"Sometimes it's hard to distingush parenchymal nodules from pleural thickening," Romano explained. However, she added, most such findings would have been miscategorized using both protocols. Also, there were also a few artifacts (3-8, avgerage 3.21, mostly beam hardening), in the ultra-low-dose images, but they did not impede nodule detection significantly, she said.
"Multislice CT at chest x-ray dose represents a promising CT imaging technique that leads to a dose reduction of 93.3% without compromising PN detection or characterization," Romano concluded.
The ultra-low-dose protocol is not routine at her institution, Romano wrote in an e-mail to AuntMinnie.com, but it is used as an alternative to chest films or chest CT in some cases, especially in younger patients. The facility does not perform CT lung screening.
"Patient enrollment is still going on, and we plan to examine about 200 adult patients," she wrote. "Moreover, we are planning to compare the diagnostic confidence and sensitivity plus specificity for pulmonary nodule detection and characterization in three different readers" -- an experienced radiologist, a radiology resident, and a CAD system.
The results should serve to highlight any differences in readers' skills, and determine whether CAD systems are suitable for the detection and characterization of pulmonary nodules at very low doses, she said.
By Eric Barnes
AuntMinnie.com staff writer
December 13, 2004
Related Reading
Lung cancer screening spots lesions early, gives patients additional longevity, December 6, 2004
Diagnostic work-up of CT-detected lung cancer variable, November 22, 2004
Web site promotes lung cancer awareness among women, November 9, 2004
CAD gets role in new ELCAP lung study, April 29, 2004
Lung CAD makes strides in nodule detection, January 30, 2004
Copyright © 2004 AuntMinnie.com