Nearly 10% of patients screened with virtual colonoscopy require a third scan position known as decubitus positioning in addition to prone and supine, according to a new study of more than 5,000 screening subjects. Decubitus scans are most often needed when colonic insufflation is suboptimal in the sigmoid colon.
Well-performed virtual colonoscopy (also known as CT colonography or CTC) is an effective colorectal cancer screening technique that is equivalent to optical colonoscopy for detecting colorectal adenomas, wrote Perry Pickhardt, MD, and colleagues from the University of Wisconsin in Madison in a study published in Abdominal Imaging. But the technique is dependent on a number of technical factors, such as optimized colonic distention, to maintain quality.
The American College of Radiology (ACR) virtual colonoscopy protocol specifies two image series -- prone and supine -- to allow complete evaluation of the colon and the shifting of dependent luminal fluid within the colon for adequate evaluation.
However, "in a minority of cases, the same colonic segments will be collapsed on the standard positions, necessitating a third series to achieve full diagnostic evaluation," Pickhardt and colleagues wrote. "The sigmoid and/or descending colon account for the great majority of nondiagnostic segments, necessitating a right lateral decubitus series to complete the examination" (Abdominal Imaging, December 24, 2010).
"The rate at which a third series is acquired at CTC is currently unknown but has important implications for quality measures, radiation dose, procedural efficiency, and training," they wrote. "The purpose of this study was to determine the rate and associated factors for acquiring a third series at CTC."
The group looked at CTC examinations from 6,380 adults (mean age, 57.4 years ± 7.8; 54.7% women) performed at three centers (more than 90% in a single large academic hospital); all data were read centrally at a single institution. The retrospective analysis included primary screening subjects and patients referred for CTC due to previous incomplete optical colonoscopy. Patients were categorized according to study indication, practice site, age, gender, body mass index, and other factors.
At all sites, the CT technologist, occasionally with input from the radiologist, determined the need for a decubitus image series, the authors wrote.
Virtual colonoscopy was performed on 8- or 16-detector-row scanners (LightSpeed series, GE Healthcare, Chalfont St. Giles, U.K.) using 1.25-mm collimation, 1-mm reconstruction intervals, 120 kVp, and either a fixed tube current-time product (50-75 mA) or dose modulation. Scanning followed cathartic bowel preparation and automated colonic insufflation with CO2 (ProtoCO2l, Bracco Diagnostics, Princeton, NJ) except for some 400 cases insufflated manually using room air.
"The main criterion for performing a third (decubitus) series is when both the supine and prone views are truly nondiagnostic at the same anatomic location due to complete or near complete focal luminal collapse," the authors wrote. "In practice, however, a CT technologist may obtain a third series when focal distention is suboptimal but arguably 'diagnostic' according to an experienced radiologist, making this determination somewhat subjective, which is unavoidable in clinical practice."
 |
 |
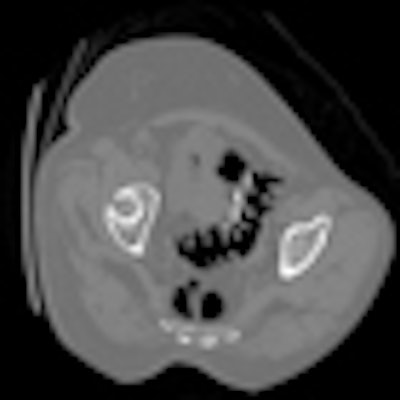
| The supine (top) and prone (above) CTC images show areas of overlapping luminal sigmoid collapse, which could result in a nondiagnostic exam. The right lateral decubitus view (below) shows good distention of the sigmoid colon, which salvages diagnostic evaluation. All images courtesy of Perry Pickhardt, MD. |
 |
Borderline cases are necessarily subjective, and the decision of whether or not to perform a third series varies according to experience and interpretive confidence, they added.
"To implement a successful CTC screening program in a busy practice, we believe that delegating this quality assurance responsibility to the CT technologists is essential," they wrote. "However, this study suggests that ongoing training and continued feedback may be important to keep the decubitus rate at an acceptable level."
Radiologists offered more input in the early years, when technologists were less experienced, but the technologists' need for oversight diminished over time, according to the researchers.
The overall rate for an additional decubitus series, regardless of indication, was 10.6% (676 of 6,380), the authors noted. However, the decubitus rate was significantly lower for exams performed for primary screening, at 9.7% (578 of 5,952), compared to exams performed after failed optical colonoscopy, at 22.9% (98 of 428) (p < 0.001). In addition:
- The need for a third position did not differ significantly by gender, at 10.3% (283 of 2,736) for men and 9.2% (295 of 3,216) for women (p = 0.190).
- Importantly, the rate progressively increased with age, from 5.0% for those younger than 50 to 28.0% for those older than 80.
- There was a strong correlation between the need for an additional series and increased body mass index (BMI), rising to more than 25% for BMI greater than 40. The decubitus rate was increased for overweight and obese individuals (524 of 4,134; 12.7%) compared to the normal weight group (108 of 1,875; 5.8%).
- Marked temporal variation in the need for decubitus imaging was found at the academic center, with quarterly rates ranging from 0 to 17% of all exams.
"When radiologists make the online decision for performing an additional decubitus view, we believe this rate can be kept under 10% for CTC screening," Pickhardt and his team wrote. "Keeping this rate under 10% will likely be more challenging when CT technologists determine the need for an additional series, as is the case for our program."
The rate also increases for diagnostic VC performed after incomplete colonoscopy, owing to a "significant increase in the anatomic challenges of redundancy, tortuosity, and diverticular disease," the group wrote.
Fewer than 1% of all cases are nondiagnostic due to incomplete distention, "suggesting that the decubitus view is salvaging a number of potentially borderline cases," they wrote.
The need for a third series increased steadily with age. A likely explanation for this trend is the increasing frequency of diverticular disease in older patients, particularly involving the sigmoid colon. In addition, the bowel wall changes associated with myochosis and perhaps spasm can result in bowel collapse or suboptimal distention.
The need for a decubitus series rose with BMI, and it was also higher in underweight individuals, who may have intra-abdominal crowding due to lack of intraperitoneal fat. Of note, the rate of incomplete colonoscopy is also higher in individuals with low BMI.
The addition of a third series increases the typical radiation dose of 5.0 mSv for prone and supine series to approximately 7.5 mSv. While this level is probably not clinically relevant, programs should be implemented to limit their use as much as possible without affecting diagnostic quality, the authors wrote.
"Our experience has taught us that segmental sigmoid underdistention is by far the most common culprit of inadequate distention," they wrote.
The effect of spasmolytic agents such as glucagon and buscopan could not be evaluated because these agents were not used in the exams. But the authors said their goal of establishing some kind of benchmark for the use of a third series had been met.
"The frequency for performing a decubitus series at CTC in our practice varied considerably according to study indication, practice site, patient age, BMI, and over time," Pickhardt and colleagues concluded. "The decubitus rates were similar between men and women. When considering our findings, it is critical to note that the CT technologist is primarily responsible for determining the need for a decubitus series -- not the radiologist."
The study results have important implications for clinical practice, including the need for improved training and feedback for CT technologists, they wrote. Future improvements in technique and training will likely reduce the need for a third series in virtual colonoscopy.
By Eric Barnes
AuntMinnie.com staff writer
February 9, 2011
















