It won't be the last word in the competition to supplant conventional coronary angiography, but the first published comparison of MRI versus multidetector CT for evaluation of coronary artery stenosis gives the lead to the former.
CT partisans may discount the study for its use of yesterday's cutting-edge, a four-slice scanner. But the researchers also state that both modalities perform well for a potentially useful role: that is, ruling out coronary artery disease in symptomatic patients who could then be spared the risks and expense of invasive angiography.
The head-to-head study, led by cardiologist Bernhard L. Gerber and radiologist Emmanuel Coche of the Cliniques Universitaires Saint-Luc in Brussels, Belgium, has been published online and is slated for print in the next issue of Radiology (January 2005, Vol. 234:1).
Several earlier published studies have looked at either MRI or MDCT, and come up with similar performances by the two modalities, the authors noted. "Yet, to our knowledge, until now, there has been no direct comparison of these two imaging approaches in the same patients," they wrote.
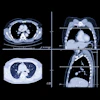
The researchers examined 26 patients with four-slice MDCT and 3D navigator-gated free-breathing MRI -- in random order on the same day -- followed by invasive coronary angiography an average of five days later. All the patients had been referred for nonurgent angio during the nine-month study period in 2002.
Both MRI and MDCT encountered some challenges in visualization, the authors noted.
"On average, image quality was judged to be better with MR imaging than with multidetector row CT (mean image quality grade, 3.6 ± 1.6 versus 3.1 ± 1.2; P < 0.001), particularly in the major epicardial arteries," they wrote. "In contrast, the side branches were generally better seen, albeit not significantly so, at CT than at MR imaging."
In addition, "the number of coronary artery segments with poor image quality (grade < 3) was higher at CT than at MR imaging (99 versus 50 of 294 segments, P < 0.001)," wrote the authors, who cited the presence of reconstruction artifacts in the right coronary artery as the problem in 46% of the cases.
"On the other hand, low CNRs (contrast-to-noise ratios) measured in the diagonal and marginal branches often resulted in poor image quality in the depiction of these segments at MR imaging."
Quantitative coronary angiography (QCA) results were used as the standard against which the MDCT and MRI findings were measured. Two readers independently reviewed the CT and MR studies, achieving an interobserver agreement of 87% on the MRI and 81% on the CT prior to arriving at a consensus interpretation.
According to the QCA results, 21 of the 26 patients had significant coronary artery disease. Out of 294 coronary artery segments larger than 1.5 mm in diameter, 58 segments (20%) had significant (> 50%) stenosis.
When compared with QCA, the noninvasive exams were split on their strengths. MDCT showed statistically significant higher sensitivity in detecting stenoses, identifying 79% of the 58 segments versus MRI's 62% rate.
But MRI showed significantly higher specificity in correctly excluding stenosis, achieving an 84% rate in 236 segments compared with CT's 71%.
Both modalities achieved a similarly high negative predictive value -- 90% for MRI and 93% for CT -- and a similarly low positive predictive value -- 49% for MRI and 40% for CT.
Overall, the diagnostic accuracy of MR imaging was 80% (correct for 234 of 294 segments) and was statistically significantly higher than MDCT's 73% (214 of 294 segments).
"The salient finding in the present study was probably the observation that despite having similar overall diagnostic accuracy in the detection of significant CAD, MR imaging and multidetector row CT significantly differed in their capability to depict diseased and nondiseased segments," the authors wrote.
"The higher sensitivity of multidetector row CT was undoubtedly related to the better spatial resolution and higher CNRs. It also probably reflected the greater capability of CT to depict calcified plaques, which usually generate a strong signal on multidetector-row CT images and are therefore quite easily identified," the authors continued.
"On the other hand, MR imaging had greater capability to depict normal or nonsignificantly diseased vessels and thus had better specificity than multidetector-row CT. This probably reflected the greater propensity of the CT findings to lead to overestimated stenosis severity, particularly in the presence of coronary calcium, which causes blurring of the vessel lumen."
As for earlier papers that found higher specificity for MDCT, the authors stated that the discrepancy was likely explained by the exclusion of nonevaluable segments from the analysis in other studies.
"The present study results show that neither MR imaging nor multidetector-row CT is ready to be a replacement for conventional coronary angiography at this time," the authors concluded.
However, "the findings nonetheless suggest that these modalities may be able to compete with other noninvasive examinations that are used to detect CAD, such as exercise stress testing," they wrote.
"Because of their high negative predictive value, MR imaging and multidetector-row CT might be particularly useful in helping to rule out the presence of significant CAD and thus avoid the acquisition of unnecessary coronary angiograms in patients in whom exercise electrocardiography might have high false-positive rates."
By Tracie L. Thompson
AuntMinnie.com staff writer
December 20, 2004
Related Reading
CT and MRI taking over x-ray's volume, report says, November 16, 2004
Coronary stents: Safe with MRI, evaluable with CTA, November 10, 2004
Is MRI the new gold standard for assessing myocardial viability? November 9, 2004
Preliminary results of MRI angiography show reliability in detecting CAD, April 7, 2003
Copyright © 2004 AuntMinnie.com











![Representative example of a 16-year-old male patient with underlying X-linked adrenoleukodystrophy. (A, B) Paired anteroposterior (AP) chest radiograph and dual-energy x-ray absorptiometry (DXA) report shows lumbar spine (L1 through L4) areal bone mineral density (BMD). The DXA report was reformatted for anonymization and improved readability. The patient had low BMD (Z score ≤ −2.0). (C) Model (chest radiography [CXR]–BMD) output shows the predicted raw BMD and Z score in comparison with the DXA reference standard, together with interpretability analyses using Shapley additive explanations (SHAP) and gradient-weighted class activation maps. The patient was classified as having low BMD, consistent with the reference standard. AM = age-matched, DEXA = dual-energy x-ray absorptiometry, RM2 = room 2, SNUH = Seoul National University Hospital, YA = young adult.](https://img.auntminnie.com/mindful/smg/workspaces/default/uploads/2026/04/ai-children-bone-density.0snnf2EJjr.jpg?auto=format%2Ccompress&dpr=2&fit=crop&h=167&q=70&w=250)



