Studies have shown that quantifying 18F-FDG kinetics with dynamic PET data can characterize many lesions more accurately than a single static measurement of uptake. The routine clinical use of dynamic PET, however, has been precluded by the long scanning time required.
Now researchers in Germany say they have identified a modified, short acquisition protocol that generates more information than standard uptake values (SUVs) and accurately estimates 18F-FDG kinetics (Journal of Nuclear Medicine, December 2003, Vol. 44:12, pp. 1933-1939).
The new protocol may be useful in evaluating a variety of cancer patients, according to Dr. Ludwig G. Strauss, Dr. Antonia Dimitrakopoulou-Strauss, and Dr. Uwe Haberkorn from the German Cancer Research Center in Heidelberg.
Among their suggested applications for short-protocol dynamic PET: detection or grading of soft-tissue sarcomas, differentiation of benign and malignant bone lesions, and assessment of therapy response in patients with metastatic colorectal carcinoma.
The authors have spent years identifying the enhanced information offered by dynamic PET. With this latest study, they wrote, "A main aim was to reduce the number of frames for the data acquisition in order to achieve a protocol suitable for routine application. Our results showed that a short, 10-minute acquisition followed by a late static image 56–60 minutes after tracer injection provided accurate data for estimating 18F-FDG influx and the parameters k1 (rate constant) and VB (vascular fraction)."
The researchers based their conclusions on 151 dynamic datasets obtained from 60 patients referred for 18F-FDG PET for primary tumor diagnostics or evaluation after chemotherapy. Both tumors with high metabolic activity and scar tissue were included in the evaluation.
To see whether a short acquisition protocol could yield more information about 18F-FDG kinetics than simple SUV, the researchers looked at data derived from a 60-minute full dynamic acquisition.
The standard two-tissue-compartment model was used as the reference. 18F-FDG influx was calculated from the compartment data, along with vascular fraction and rate constants k1–k4. The dynamic PET data were evaluated using the PMod software package from the University of Zurich.
"We identified the contribution of the SUVs for the individual time frames of the dynamic 18F-FDG study to the quantification parameters," the authors wrote. "Based on the results, we propose a simplified method for the prediction of quantitative parameters."
The first 10 minutes of the 60-minute scans stood out, as the influx data were significantly correlated with the full scan results after just two minutes, while the VB and k1 correlation coefficients were highest less than 10 minutes after tracer injection.
No significant correlation was observed for SUV and the rate constants k2–k4, the researchers found.
 |
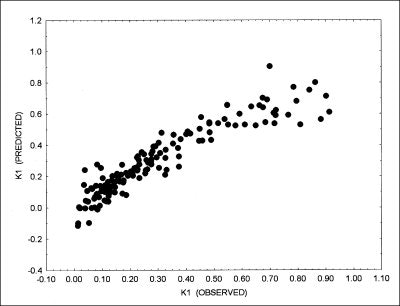
| Correlation of k1 as calculated by two-compartment model (k1 [observed] and predicted k1 (k1 [predicted]) using short acquisition protocol. Input data from 1 to 10 minutes (10 frames) and target area from 1 to 10 minutes (10 frames) and from 56 to 60 minutes (1 frame) were used for prediction, based on polynomial function (degree 2) for data fitting. Correlation coefficient of 0.9305 was obtained (republished with permission from the Journal of Nuclear Medicine). |
However, the authors noted, "a general limitation of dynamic studies is the need to focus on a single target area because of the limited field of view of current PET scanners. Therefore, appropriate a priori information must be available to select the target region for the dynamic data acquisition, particularly for multifocal disease."
Also, because patients will be repositioned nearly an hour after the 10-minute dynamic scan for the final late scan, skin markers must be used to maximize accuracy, they wrote.
As for the utility of a 10-minute dynamic scan, the authors looked to their own previous studies and others for examples. Other investigators, for example, have found k1 and influx data could differentiate teratomas where SUV or visual analysis could not.
 |
|
PET imaging reproduced in an earlier publication by the authors shows transverse (A), sagittal (B), and coronal (C) images of patient with histologically confirmed lipoma in proximal upper leg one hour after FDG injection. Low FDG uptake is evident in suspicious lesion. Cross cursor is positioned over suspicious lesion according to clinical examination. Cube shows relative position of cursor to field of view. (From "Dynamic PET 18F-FDG Studies in Patients with Primary and Recurrent Soft-Tissue Sarcomas: Impact on Diagnosis and Correlation with Grading," republished with permission from the Journal of Nuclear Medicine 2001, Vol. 42, pp. 715). |
The authors also cited their own experience using dynamic data to differentiate soft-tissue sarcomas by grade. Whereas SUV detected only 50% of grade I tumors, kinetic data "were helpful in the detection of 80% of grade I tumors and 84% of grade III tumors, as well as 50% of lipomas and 38% of grade II tumors."
"In our opinion, patients should be selected for the shortened dynamic protocol if a more-detailed quantitative analysis of 18F-FDG kinetics will likely be helpful for differential diagnostics or for assessment of the response to chemotherapy," the authors concluded.
By Tracie L. Thompson
AuntMinnie.com staff writer
December 30, 2003
Related Reading
PET/CT is the team to beat for NSCLC staging, November 17, 2003
FLT-PET shows promise in differentiating unclear lung lesions, October 1, 2003
PET detects lymph node activation during HIV infection, September 19, 2003
Trial questions PET's cost-effectiveness for Alzheimer's diagnosis, September 16, 2003
FDG-PET deemed most accurate for catching Hodgkin’s relapse, September 1, 2003
Copyright © 2003 AuntMinnie.com