VIENNA - Systemic inflammation has long been suspected of contributing to the destabilization of vulnerable plaques in acute coronary syndromes, while imaging has remained at the sidelines of the discussion. Now, however, radiologists from Italy believe they have found a link between signs of vascular inflammation on MRI and the presence of unstable angina.
In a presentation yesterday at the European Congress of Radiology, Dr. Luigi Natale from the Catholic University in Rome discussed his group’s efforts to evaluate the presence of a hyperintense signal within carotid atherosclerotic plaques of patients with angina.
"It is unknown whether multifocal plaque activity may also affect remote arterial (regions) as a result of systemic inflammatory factors," Natale said. To look for an imaging correlation, his group examined edema (and wall thickening) as a sign of plaque inflammation in patients with unstable angina related to serum levels of C-reactive protein (CRP). Finding such a correlation could lead to better diagnosis and management of patients with unstable plaque, he said.
The group examined 14 patients, 7 with unstable angina and carotid plaques with stenoses > 40% (mean age 67), and a control group of 7 patients, 5 with stable angina, and 2 without coronary artery syndrome or signs of stenosis (mean age 65).
All patients underwent angiographic examination, followed by MR imaging before and 10 minutes after administration of 0.2 mmol/kg of gadolinium-DPTA contrast. Images were acquired on a 1.5-tesla scanner using T1 and T2-weighted double- and triple-inversion-recovery black-blood spin-echo and fast spin-echo sequences (3-mm thickness, 256 x 256 matrix).
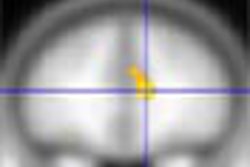
The criteria for plaque formation was defined as increased T2 signal intensity (on STIR or spin-echo images) indicating the presence of edema as a marker of inflammation, he said.
Two readers working independently evaluated the results to assess: 1) wall thickening as an indicator of arterial wall edema and/or infiltration 2) increased T2 signal intensity as an indicator of arterial wall and/or plaque edema, and 3) arterial wall and/or plaque enhancement as an indicator of increased capillary permeability. CRP levels were determined using an ELISA assay.
"Of the 10 total plaques imaged in patients with unstable angina, 8 showed increased gadolinium enhancement in T2-weighted MRI," Natale said, compared to 1 plaque in a control subject. More important, "patients with MRI evidence of inflamed plaques had threefold higher levels of CRP (mean 15.6) compared to (patients with) noninflammed plaques (mean 5.5, p < 0.05)." He concluded that patients with unstable angina exhibited signs of vascular inflammation in MRI more frequently than control subjects.
"In this small number of subjects the correlation appeared very strong," Natale said. "Our data suggest that plaque activity in acute coronary syndromes also affects remote vascular (regions), possibly mediated by systemic inflammation."
In response to a question from the audience, Natale said he has not yet seen a change in MRI results in patients who have undergone statin therapy.
By Eric Barnes
AuntMinnie.com staff writer
March 10, 2003
Copyright © 2003 AuntMinnie.com