MIAMI BEACH, FL - For obvious reasons, imaging pregnant patients with abdominal pain requires an extra degree of finesse. At present, CT, MRI, and ultrasound all have their proponents.
During a presentation Monday at the American Roentgen Ray Society meeting (ARRS), Dr. Katherine Birchard made a case for using MRI to assess acute abdominal pain in pregnancy women.
Birchard and of her colleagues are from the University of North Carolina Hospitals in Chapel Hill. Co-author Dr. Michele Brown is from the medical center at the University of California, San Diego.
"Acute abdominal or pelvic pain in the pregnant patient can be a challenge," Birchard said. "Is the pain obstetric or caused by something else?"
While ultrasound is the first choice for imaging these patients, in the presence of a gravid uterus, intra-abdominal organs are difficult to assess sonographically, she said.
The patient population for this study consisted of 23 pregnant women who were referred for imaging due to acute abdominal or pelvic pain between June 2002 and September 2003. The average age was 27 for the women and 23 weeks gestational age for the fetus. In the majority (17) of these patients, MR was the primary imaging modality; five patients had an initial ultrasound exam that was indeterminate. All of the patients were sent for MRI by the referring clinician.
First, non-contrast multiplanar multisequence MR images of the abdomen and pelvis were obtained. A radiologist then reviewed these images to determine if a diagnosis could be made without the addition of gadolinium. Thirteen out of 17 non-contrast exams were deemed acceptable. All MR interpretations were compared with medical, surgical, or obstetric records; follow-up was done until the date of final chart entry (mean of 4.1 months).
According to the results, MR correlation with medical records demonstrated the correct identification of disease entities in 16 out of 17 patients. MRI interpretation pinpointed a number of disease processes, including uterine fibroid degeneration, pancreatitis, simple ovarian cysts, and bilateral adrenal hemorrhage.
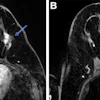
One patient at 31 weeks gestation presented with acute pain in the lower abdominal cavity. She was diagnosed with appendiceal abscess based on the MR exam. Surgical intervention revealed pus and a perforated appendix; she delivered at 29 weeks, Birchard said.
In another example, the patient (21 weeks gestational age) had right lower quadrant pain and fever. She was diagnosed with pyelonephritis on MR, treated with intravenous antibiotics, and carried to term.
In one patient, ovarian torsion could not be identified either prospectively on MR or during a retrospective review of the records, Birchard said.
"The safety and accuracy of MR make it an excellent choice for evaluating pregnant patients," she concluded.
Session attendees were curious as to how the patients who required gadolinium were handled. Birchard said that the contrast agent was administered only with the consent of the patient, referring physician, and an attending radiologist. The group used the guidelines set out by the gadolinium manufacturer (Omniscan, Amersham Health, Little Chalfont, U.K.), which recommends against use in the first trimester. In these five cases, the contrast-based imaging protocol was determined by the quality of the non-contrast MR images, she said.
Another attendee suggested that rather than imaging the patients in a supine position, Birchard's group should consider putting them in a decubitus position with a phased-array coil over the area of interest. This would enhance the images as well as make the exam more comfortable for the patient. Birchard agreed, but added that the majority of MR scans took 20 minutes or less.
Future research should include a larger patient population as well as a comparison between ultrasound and MRI, Birchard said.
By Shalmali Pal
AuntMinnie.com staff writer
May 4, 2004
Related Reading
Ultrasound supports conservative treatment of post-conception symptoms, April 27, 2004
Limited fetal risk seen in uroradiological procedures on pregnant patients, May 1, 2003
Procedure-associated radiation exposure adds minimal risk in pregnancy, January 14, 2003
Policy clarifies imaging risks for pregnant women, May 15, 2002
Copyright © 2004 AuntMinnie.com