A centralized 3D postprocessing lab can provide a range of clinical, efficiency, quality assurance, and financial benefits. Successfully launching a centralized 3D postprocessing lab in the community practice requires navigating a broad range of practical considerations, however, according to Dr. Jay Cinnamon of Quantum Radiology in Marietta, GA, and Gordon Harris, Ph.D., of Massachusetts General Hospital (MGH) in Boston.
3D visualization enables faster and more confident diagnoses and treatment decisions, and quantitative analysis and computer-aided detection can provide more accurate and reliable treatment planning, staging, and assessment, according to Harris.
"Ultimately, the goal is improved patient care, increased clinical confidence, (and) reduced time, cost, and invasiveness," Harris said.
But before those benefits can be realized by a 3D lab in a community practice, a good strategic plan must first be formulated.
Strategic planning
Deciding on the criteria for studies to be handled by the 3D lab is important. To be handled in the 3D lab at Quantum Radiology, the postprocessing must bring added clinical value to referring clinicians, Cinnamon said. In addition, the postprocessing itself has to be complex enough that it's beyond the reasonable expertise of the CT and MR technologists, he said.
"For example, one point that differentiates (the Quantum lab and the MGH 3D lab) is that we do not bring the routine MRAs (MR angiographies) of the brain in our practice into the 3D lab," Cinnamon said. "That's done by the MR technologist at the operator's console."
Cinnamon and Harris spoke during a joint presentation at the 2007 RSNA meeting in Chicago.
Many types of studies can be brought into the community radiology 3D lab, including CT angiography (CTA), perfusion CT, musculoskeletal, virtual colonography and bronchoscopy studies, CT urography, volumetric analysis, fusion imaging, and functional analysis. In the MR domain, MR angiography, perfusion MRI, advanced neuro MRI such as tractography and functional MRI, volumetric analysis, viability studies, and fusion imaging could also be candidates for the 3D lab, according to Cinnamon.
The basic components of a 3D lab involve workstation technology and connectivity issues, processes and protocols, staffing at many different levels, technologist training, a business model, strategic and tactical planning, IT support, and quality control, he said.
In beginning the strategic planning process for a 3D lab, a good first step is to determine if you want to be more efficient or perform new clinical applications, Cinnamon said.
"It's often both," he said. "But just start thinking along the lines of 'Is this efficiency?' -- in other words, getting me from my 45 minutes for neurovascular CTA down to under 10 minutes, or is it that I don't yet do virtual colonography in my practice and I'd like to start."
Goals can then be defined in terms of scope, resources, challenges, metrics, and timeline, he said.
IT issues encompass workstation technology, IT architecture models for accessing 3D postprocessing software, and the human-technology interface, Cinnamon said.
One question that often comes up in planning for a 3D lab is how to decide on the best 3D workstation. There are many different vendors for 3D workstations, and institutions also have to choose between a workstation or distributed model, Harris said.
"Some vendors have a distributed model that has certain functions available, but not all of the functions, and you have to have the workflow (in place) to do some of the more complex things," Harris said. "Other vendors are going toward a completely integrated distributed model."
In choosing the workstation package, determine your most important applications and decide your priorities, he said. Frequency of use is also a consideration, as power users and occasional users may have different requirements.
"The more feature-rich and the more ability you have to interact with the parameters of the workstation and do complex processing, (the more) it tends to be less user-intuitive and user-friendly," Harris said. "Or do you want something that you can just get down to, spend an hour kind of learning the basics, and do what you want to do without a lot of in-depth training."
The number of users and locations will also need to be considered in determining the configuration, Harris said. If you have 10 people in different reading rooms, for example, a server-client approach may be required.
As far as staffing goes, a lab supervisor needs to be named. At Quantum Radiology, that role is filled by a technologist, Cinnamon said. Physician champions are also essential, he said.
"You can't launch this without somebody signing on and saying, 'I'll take control over virtual colon' or 'I'll take control over mesenteric CTA,' " he said. "You have to have physician champions who are going to work with the folks in the 3D lab, and obviously you have to have technologists who are specially trained."
These 3D technologists need to have familiarity with anatomy, cross-sectional imaging, and computers, Cinnamon said. In addition, they need to have certain personal traits, including being self-motivated and detail-oriented.
"The interplay between the technologists and the radiologists and referring physicians is the key to developing clinically useful 3D imaging," Harris said. "That has been the key to the success of both of our groups."
Money matters
To achieve 3D billing compliance, institutions have to follow a few rules. For separate 3D exams, the 3D exam accession number needs to be linked to the primary exam and go out together for billing, Harris said. In addition, 3D needs to be mentioned in the clinical report.
Some exams are billed separately for 3D, while others have 3D bundled in, Harris said. There are two 3D CPT add-on codes, 76376 (3D rendering with interpretation and reporting of CT, MRI, ultrasound, or other tomographic modality not requiring image postprocessing on an independent workstation) and 76377 (3D rendering with interpretation of CT, MRI, ultrasound, or other tomographic modality requiring image postprocessing on an independent workstation).
These are billed in association with the primary CT, MR, or ultrasound code, but can't be billed with CT angiography, MR angiography, or virtual colonoscopy; 3D is considered part of those procedures, Harris said.
Requirements for reimbursement include departmental protocol and physician notification of the need for 3D, a specific request from the physician, or a positive finding by the radiologist that requires further views. Processing must also be performed on software cleared by the U.S. Food and Drug Administration.
If the 3D lab is part of the hospital, the technical component is billed through the hospital, but is now considered bundled as part of the CT, MR, or ultrasound codes. If the 3D lab is part of the physicians group, then it's billed through the Medicare fee schedule, either via global or split billing, Harris said. In either hospital or nonhospital-based billing, professional reimbursement is about $41.
Operational issues
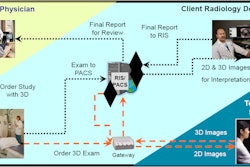
At both MGH and Quantum Radiology, imaging studies are sent from the modalities to the PACS, from there they are viewable on the PACS and through a Web-based distribution system on PCs across the enterprise. If 3D is required, that case is brought to a 3D workstation. The new 3D views are processed, and a 3D series is created and pushed back to the PACS where it's viewable as a new series with that study, Harris said.
"So whenever you view the case, you see the original series plus their new series for all of the 3D views that have been created," he said.
Developing processing and filming protocols offers a means of achieving efficiency gains. The radiologist-technologist continuum is also an important element workflow issue, and the roles of technologists and radiologists in performing postprocessing will often vary depending on the application, Cinnamon said.
Technologists can often serve as an important first set of eyes. "I don't read a CTA study without hearing what the techs in our 3D lab thought about when they interrogated the study," Cinnamon said. "I want to know their impression."
Structured reporting and protocols can eliminate the computer-related variables between radiologists, Cinnamon said. At MGH, 3D protocols are incorporated right into the scanning protocols, and are listed in the departmental policy and procedure manual, Harris said.
It's also important to have quality control in the 3D lab, including evaluating the accuracy of physician interpretations, quality of postprocessing by technologists, and the quality of scan acquisition, Cinnamon said. On the technology end, it's a good idea to examine the quality of the software, and perhaps correlate, for example, coronary artery CTA studies with cardiac cath findings to determine if a diagnosis of significant stenosis was actually correct, he said.
"You don't wait for something to clearly be broken before you launch a QA initiative," Cinnamon said. "Anything that seems that it might be broken you (should be) already proactively starting to investigate to see whether or not it truly is broken and what you need to fix. You can make the argument that anything new you do in your practice you should simultaneously launch a metric analysis for quality control."
Marketing
Once the 3D lab is up and running, it's important to get the word out and secure support from radiologists and referring physicians throughout the enterprise, Harris said.
"It does requires communicating what you can do and what it is that you are doing, and getting relationships built (based) on what people's needs are," he said. "Marketing of your 3D services is very important to build your 3D lab."
At the same time, growth needs to be managed in a manner appropriate with your capacity, Harris said.
"If you start offering all kinds of stuff and you don't have the infrastructure to deliver it, you start to overpromise what you can do," he said. "Ultimately, you have to maintain the quality and timeliness of your service."
Marketing the service can be done in multiple ways, including getting profiles in local newspapers and marketing to and enlightening physicians with cases that could benefit from 3D, according to Cinnamon.
By Erik L. Ridley
AuntMinnie.com staff writer
February 19, 2008
Related Reading
Hybrid lung segmentation software boosts performance, February 13, 2008
Radiologists more likely to reject certain true-positive CAD findings, January 22, 2008
3D CT planning organizes acetabular fracture fragments into a surgical framework, December 24, 2007
CAD may boost radiologists' ability to characterize lung nodules, November 25, 2007
Copyright © 2008 AuntMinnie.com