No one disputes the importance of delivering diagnostic test results as rapidly as possible to the physicians who order them. From the perspective of a radiology or laboratory department, conveying critical results to clinicians are among its top priorities.
Historically, this hasn't been foolproof -- far from it. Documented incidents and anecdotal stories abound concerning breakdowns in communication and failures to get urgent test results to caregivers.
Healthcare IT vendors have developed critical test results management (CTRM) software to help simplify, streamline, and make more foolproof the delivery of urgent information, but CTRM implementation often meets with resistance in hospital environments.
To date, CTRM software has not been deployed in large quantities. Based on input from manufacturers, AuntMinnie.com estimates that there are fewer than 400 installations in U.S. hospitals.
Hospital by bed size
 |
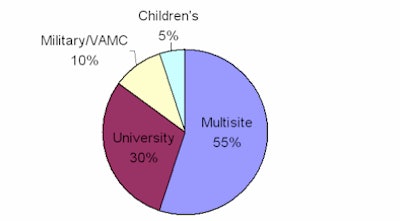
Hospital by facility type
 |
| Hospital use of CTRM for reporting critical results of patients' exams to referring physicians. Data provided by Nuance Communications. |
Joint Commission requirements
Joint Commission audits now require facilities to prove they have a mechanism for documenting and monitoring the delivery of critical test results. For many radiology departments, life changed on January 1, 2004, when the Joint Commission implemented its National Patient Safety Goals initiative. One of the goals -- to improve the effectiveness of communication among caregivers -- included the requirement to "measure and assess, and if appropriate, take action to improve the timeliness of reporting, and the timeliness of receipt by the responsible licensed caregiver, of critical tests and critical results and values."
Hospitals were required to formally:
- Define the meaning of a critical test and a critical result or value
- Define the acceptable length of time between the ordering of critical tests, performing the critical tests, and the reporting of them
- Define the acceptable length of time between the availability of critical tests and delivering them to the responsible licensed caregiver
- Show documentation that the recipient of the results repeated them accurately to the deliverer
- Collect data on the timeliness of the process, determine if there is a need for improvement, and identify methods to do so
All of this required documentation. During a survey, the Joint Commission will audit one or several randomly selected days to evaluate the number of critical test results reported out of the total number of diagnostic results, and the method by which they were conveyed. The audit also will assess whether the established standards referenced above are being met.
This has led to increased interest by hospitals to bite the bullet and install software to manage CTRM reporting. But it's not as simple as writing a request for proposal and making a purchase. The following examples illustrate how a few healthcare providers have implemented and benefited from CTRM software.
St. Joseph's/Candler Hospitals
St. Joseph's/Candler is a healthcare system with two community hospitals located in Savannah, GA. Its 10 radiologists interpret approximately 207,000 diagnostic imaging procedures a year. Prior to the implementation of CTRM software, the process was time consuming and labor intensive, according to Jeffrey Zehel, director of imaging.
The site relied on a radiologist to note the date and time on his final report that a critical result was successfully delivered, and while radiologists tried to comply, the information didn't get recorded 100% of the time. If a radiologist couldn't reach the referring physician, or if the referring physician didn't respond to a phone message, other members of the radiology department would take over, according to Zehel.
"We could spend hours on the phone trying to track the doctors down and still not succeed," he said. "Sometimes we would call a physician's nurse or their office and leave a message."
The following day, an average of four hours would be spent by trained clerical staff or by the PACS support team to review all of the reports to identify the ones with critical results. A critical findings list of 20-22 entries would be compared against the reports. Of those that were identified, it was then necessary to verify that the critical results had been reported and to determine if this had been done within or outside the hospital's guidelines.
"The process was laborious, time consuming, and not always 100% accurate, in spite of best efforts," Zehel explained. "Additionally, we had no way to automate and report this within the RIS."
Zehel had seen a demonstration of an automated CTRM system (Veriphy, Nuance Communications, Burlington, MA) and assembled a team of key physicians including the radiology department chairman, the vice president of IT, and an emergency physician to evaluate the system. It took approximately four months to build the database of referring physicians with respect to obtaining preferences for notification and all of the associated contact numbers.
The system was tightly integrated with the installed PACS (Sectra, Linköping, Sweden) and the speech recognition system (PowerScribe, Nuance), which made it easier to use because only a few additional buttons needed to be clicked, according to Zehel.
However, an unexpected problem that arose was interaction with emergency physicians. Located literally across the hall, they expected to be telephoned or to have a radiologist walk across the hall. The CTRM system originally did not have a way for the radiologists to report this interaction.
The software was modified to enable a radiologist to push a "documentation only" button and verbally dictate the time and method by which the information was delivered, as well as verify that the results had been acknowledged and repeated by the recipient. This data was recorded into the system.
University of Colorado Hospital
The University of Colorado Hospital failed at its first attempt to implement a CTRM system. Its experiences represent the classic example that physician buy-in is absolutely critical to succeed and that implementation should not take place when other major activities are occurring.
At the recent American Healthcare Radiology Administrators (AHRA) annual meeting, RIS/PACS administrator Michael Cain from the University of Colorado Hospital explained how his initial efforts to install CTRM software were bogged down by external factors -- the installation of a new PACS network and the hospital's move to an entirely new campus.
The IT department signed a contract for a new PACS and for a CTRM software system just eight months before a scheduled move from the hospital's downtown Denver facility to a sprawling campus in nearby suburban Aurora. As a result, clinical staff were simply too distracted by the move to learn the new CTRM system.
After the hospital moved and the staff had settled into the new campus, Cain tried again, and the CTRM program was officially relaunched in 2008. While the implementation is proceeding more smoothly this time, there are still kinks to be sorted out, such as the complexity of forms required to define the software's preferences and protocols for notification of physicians and residents.
Approximately 10-12 critical results need to be conveyed, mostly during the day, with approximately one-third designated for the emergency department. The efficiency of the emergency department, with a single telephone number answered promptly 24/7 by an emergency physician, has made the CTRM system impractical for radiologists. It added additional steps to the reporting workload, because like the radiologists at St. Joseph's/Candler, they had to formally report information about delivery of critical results.
To increase reporting compliance, the software has been integrated with the speech recognition system. A simple and fast three-step process -- click to open the application, dictate, and click to close -- generates more but not all usage.
Another notification challenge was generated by the fact that hundreds of residents at the University of Colorado Hospital order diagnostic procedures. It was necessary to meet individually with the medical directors for all services so that the radiology department could be provided with a backup contact for every resident.
The system was initially configured to have the originating radiologist notified if a referring physician failed to respond within the 60-minute compliance period. This was a mistake, according to Cain, because it was very disruptive to the radiologists' workflow. The system was changed so that a designated member of the radiology staff would receive the notification and be responsible for tracking someone down.
Even this can be onerous and disruptive, however, and if there is no response after three paging attempts, the system automatically converts to a remote, 24/7 manned vendor support team that provides live backup notification to its customers. This remote team spends the next 60 minutes trying aggressively to reach a clinician. If it fails to do so after that point, the on-call radiology administrator is paged, and they call the house manager. This happens three to four times weekly, according to Cain.
"Implementing a CTRM system in a large hospital requires that senior-most executive management make a commitment to the project and convey this as much as necessary," Cain said. "You don't realize how big a job it is to make the system work, and you need to plan lots of time communicating at all levels, repeatedly. It is imperative to get the buy-in of all the doctors to achieve the efficiency that the system is designed to deliver."
Plaza Medical Center of Fort Worth
More than 1.2 million laboratory tests are performed annually at Plaza Medical Center of Forth Worth, TX. Of these, there are 1,500 critical results a month to report.
The 320-bed community hospital was successfully using CTRM software for its radiology department, so it acquired laboratory reporting software as soon as it became commercially available, according to laboratory manager JoAnne Beveridge. Executives responsible for quality control and patient safety made the decision to purchase and implement. As one of approximately 10 hospitals in the country using Veriphy Lab software, it's a very early adopter.
The system saves hours of time for the department's technical staff of 45, Beveridge said. The application is on every desktop, and all the staff has to do is type the patient's name, select the nursing unit, select the physician, and put in the results.
"Before implementation, it was not uncommon for each of our staff to be placed on hold for up to 20 minutes," Beveridge said. "Our lab was filled with 'on-hold' music coming from the speakerphones, which also could be disruptive."
There were glitches. Physicians who rarely ordered diagnostic imaging procedures were finding themselves inundated with critical results notifications from the laboratory. Many wanted to opt out of the system, which was not allowed. Many then opted to change their process of notification from a cell phone, text message, or pager to having the notification sent directly to the office. In these situations, licensed nurses tend to be the individuals designated to receive and read back the results, which are recorded automatically in the CTRM system.
An internal problem that has yet to be completely resolved is that when a critical test result is faxed and/or telephoned to a nurses' station in the hospital, the nurse will hand it off to a resident, who doesn't complete the documentation trail.
Getting documented closure is an issue. The CTRM software has added the unplanned step of a lab staff member reviewing the files of a patient's electronic medical record to determine if the results were acted upon when notified that the compliance period has passed. If they were, the lab staff member documents this in the CTRM system. If there is no evidence, it's necessary to proceed to the next escalation level. Both of these steps, based on failure to cooperate with the system's rules, add work for the lab team and reduce the efficiency of the system.
In conclusion, it takes a lot of work and the commitment of end users to make CTRM software a success. How rapidly will this technology be adopted? What additional features will improve acceptance by end users? It's anyone's guess.
By Cynthia Keen
AuntMinnie.com staff writer
September 22, 2008
Related Reading
Software boosts delivery of critical radiology results, July 17, 2008
Autofax reporting breakdown spurs Calgary headlines months later, March 19, 2008
Copyright © 2008 AuntMinnie.com


















