BOSTON - Multislice CT and whole-body MR are the modalities of choice for imaging patients with multiple injuries in level-one trauma centers or tertiary-care hospitals. These modalities are able to provide radiologists with the necessary tools to rapidly diagnose the extent of trauma. However, the task of associating relevant images from these studies in a PACS with each of the requested procedures from a RIS can be difficult and time-consuming.
"We generate approximately seven million CT images on an annual basis, and we’ve had as many as 4,500 images on a single exam," said Dr. Gary Wendt, a neuroradiologist at the University of Wisconsin in Madison. "Searching for relevant images within a dataset this large can be extremely frustrating for both the radiologist and the referring clinician."
Wendt presented the results of an implementation of the Presentation of Grouped Procedures (PGP) integration profile at his facility at the Symposium for Computer Applications in Radiology on Saturday.
The PGP profile, which is described in the Integrating the Healthcare Enterprise (IHE) initiative Technical Framework v.4.6 (Year Three), is a method to address multiple requested procedures performed in one grouped acquisition.
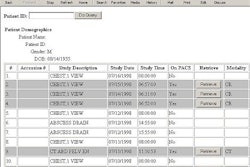
According to Wendt, there are two informatics problems that occur when multiple requested procedures are performed in a single acquisition. One is that, although a RIS lists several study procedures for various anatomical regions, there is only one study listed in a PACS, and several reports must be generated from the exam.
The second problem occurs when one radiologist marks a study as "read" in a PACS. Radiologists who will be reading the other procedures will no longer see the exam in their in-box, requiring them to search for the relevant images for their requested procedure throughout the entire dataset.
In a trauma situation, where there are often many subspecialty exams performed in one scan, these problems are magnified, he said.
"Obviously, you can’t deal with this type of problem in the film environment, unless you’ve got alternating alternators," quipped Wendt.
To implement PGP at the institution required a combination of modality and PACS modifications. The CT units (GE Medical Systems of Waukesha, WI) had a post-acquisition application added that created image subgroups as well as grayscale presentation states. The PACS products (McKesson Information Solutions of Richmond, BC, and UltraVisual Medical Systems of Madison, WI) had a software modification to support the PGP information passed from the modalities.
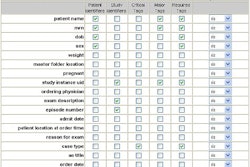
The PACS now implements virtual image splits by receiving PGP information as grayscale presentation suite (GSPS) objects. As a result, Wendt said, PACS users are presented with only the relevant images for a body part selected in an exam and the PACS only needs to keep one dataset with all the acquired images.
Wendt cautioned that PGP is not a trivial implementation and that it requires vendors to cooperate and implement lab-to-lab testing to ensure proper functionality before clinical implementation. Technologist workflow, for example, may have to be altered to implement PGP availability.
"At the present time, our RIS cannot track orders from the PACS as they’re performed. Our technologists now have to go to a separate workstation in order to enter the information, which is not the most efficient use of their time," he said.
By Jonathan S. Batchelor
AuntMinnie.com staff writer
June 8, 2003
Copyright © 2003 AuntMinnie.com