A New Jersey state x-ray quality assurance program has yielded improved image quality and lower radiation doses, according to research from the New Jersey Department of Environmental Protection and the University of Utah Health Sciences Center in Salt Lake City.
"This is a successful program with no downside, and I’m going to be surprised if we don’t see similar legislation from other states in the very near future," said Dr. William Orrison, Jr. of the University of Utah Health Sciences Center. Orrison presented the research, conducted with Jill Lipoti, Ph.D., assistant director, radiation protection programs at the New Jersey Department of Environmental Protection, at the 2003 RSNA meeting in Chicago.
Shifting to an outcome-based inspection approach that focuses on image quality and entrance skin exposure (ESE), the New Jersey radiation control program implemented a new regulation, Quality Assurance Programs for Medical Diagnostic X-ray Installations, in January 2001. Under the regulation, all hospitals and medical chiropractic and podiatric offices employing diagnostic medical x-ray equipment (including radiography, fluoroscopy, x-ray bone densitometry, and CT) were required to establish and carry out a quality assurance (QA) program.
Affected facilities included 3,542 sites, comprising 94 hospitals, 1,494 medical offices, 1,293 chiropractors, 626 podiatrists, and 35 industrial, school, and government facilities, Orrison said.
The purpose of the program was to reduce unnecessary radiation, provide more timely equipment repair and less downtime, and improve image quality, resulting in better diagnoses and fewer repeat x-rays, Orrison said. Program designers also hoped the program would lead to improved understanding of x-ray risks and benefits, as well as closer ties with constituents.
"There’s a need for some improvement," he said. "Quality assurance in a systematic approach is the only way we’re going to get there."
Quality control (QC) tests, frequencies, and standards were specified, and as an aid, four compliance guide documents were prepared: Quality Assurance Manual, Radiographic Quality Control, Fluoroscopic Quality Control, and CT Quality Control.
The QA program measures patient radiation exposure and requires periodic QC tests. It also evaluates processor functionality and image quality, and includes an annual system analysis by a qualified medical physicist.
Positive results from federal regulation of mammography via the Mammography Quality Standards Act (MQSA) actually paved the way for the program, serving as a model, Orrison said.
"The MQSA program led to significant reduction in radiation dose and significant improvement in image quality for mammography," he said. "The question (was): Could we apply those same standards or similar standards to general imaging?"
The research project was performed to assess the two-year outcome of the new regulation, which included a goal of 10% reduction of ESE. State inspectors visited each facility, taking a phantom image and scoring it using a variety of criteria. The facility’s QA program was also audited.
ESE was measured for three procedures: AP foot radiography, PA chest radiography, and AP lumbar spine radiography. Before the program was implemented, mean ESE for the foot study was 33.8 mR; in the first year of the program that dipped 48% to 17.5 mR, and in the second year, declined 68% to 10.5 mR.
The chest study ESE was measured at a mean of 25.5 mR prior to the program, at 16 mR (down 37%) in the first year of the program, and at 13.8 mR (down 46%) in the second year. Lumbar spine exam ESE came in at 582 mR before the program, 466 mR (down 20%) in the first year, and 367 mR (down 37%) in the second year, according to the study team.
The goal of a 10% reduction in ESE was exceeded in the first year, and the current dose reduction for New Jersey patients has reached over 35%.
Image quality
The program also had the goal of improving image quality by 15% for all diagnostic procedures by 2007. From the phantom, image quality tests were performed, with scores given for different criteria. Inspection information is entered into a computer database; a report is generated and sent to each facility.
This report scores each of the tests as excellent, good, fair, or poor, and provides an overall score of the image quality. The relative weight of each criterion was background density (25%), high contrast resolution (20%), noise/artifacts (20%), density uniformity (10%), low contrast resolution (10%), low contrast detail (10%), and film contrast (step wedge) 5%.
Minimum levels for adequate images were judged as:
- Background density: 0.8 to 1.8 O.D.
- High contrast resolution: 2.0 lp/mm
- Noise/artifacts: moderate
- Density uniformity: moderate
- Low contrast resolution: three of eight holes
- Low contrast detail: two pair of holes
- Film contrast (step wedge): 0 steps
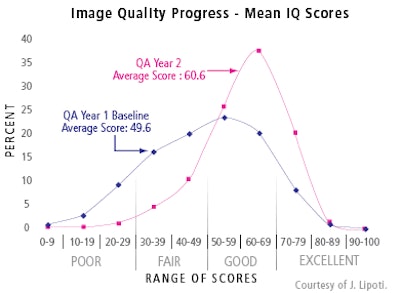
Baseline mean data taken from year 1 (April 15, 2001 to September 11, 2002) of the QA program were compared with data from year 2 (September 12, 2002 to September 12, 2003). In the first year, the average QA score was 49.6, compared with an average score of 60.6 in year 2.

The number of sites generating poor image scores was 11% in year 1, and only 2% in year 2. Good-to-excellent images were reported from 53% of sites in year 1, and from 83% in year 2.
Facilities with poor image quality scores were asked to consult with their physicist, determine the cause, make changes, and send a report of their findings and corrective actions to the state within 30 days, said Lipoti, who served as the lead author.
The original goal of improving image quality by 15% for all diagnostic procedures by 2007 has also been exceeded.
"Overall there has been a 22% increase in average image quality scores," Lipoti said. "More importantly, there has been a decrease in the number of facilities producing poor images."
Lipoti noted that the few facilities that have run into compliance problems were primarily those that failed to carry out the quarterly, semiannual, and annual tests.
"Quality assurance programs are not a one-time event," she said. "To ensure continuous, high-quality radiography, quality assurance needs to be followed continuously. When it is, the successes are obvious."
Lipoti credited bureau manager Paul Orlando and his team of nine x-ray inspectors for the success of the program.
"Many states have programs to inspect x-ray machines, but I think that New Jersey is unique in requiring quality assurance as a means to reduce entrance skin exposure while maintaining (and enhancing) image quality," she told AuntMinnie.com in an e-mail. "The involvement of medical physicists in the development and implementation of the program was essential to its success."
By Erik L. RidleyAuntMinnie.com staff writer
January 23, 2004
Related Reading
Investigators find x-ray dose reduction varies widely among digital mammo machines, December 3, 2003
Pediatric CT won't stop growing, but dose can be minimized, May 8, 2003
DR permits lower chest dose than film or CR, January 30, 2003
Worrisome radiation dose seen in CT lung screening, follow-up, December 23, 2002
No compromise in breast image quality with lower FFDM dose, December 13, 2002
Copyright © 2004 AuntMinnie.com