This article originally appeared in the American Journal of Roentgenology, written by Dr. Howard Forman, associate editor of health policy for the American Roentgen Ray Society (ARRS).

Collaborators at the American College of Radiology (ACR), many former and present medical students and residents, and I have devoted considerable time since 1998 to analyzing the radiology job market.
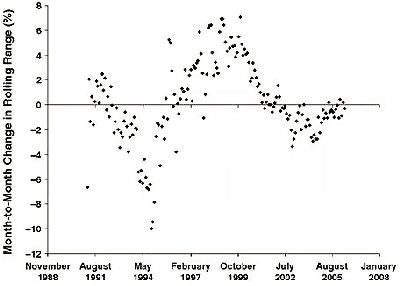
In our first publication on the subject in early 2000 (American Journal of Roentgenology, April 2000, Vol. 174: 4, pp. 933-938), we presented our Help-Wanted Index from 1991 through 1998. This index included the number of positions advertised in the AJR and Radiology. Recently, these data were updated (see figure below).
 |
| Image from AJR, September 2006, Vol. 187:3, pp. W249-W254, courtesy of ARRS. |
Those of us in clinical practice during those years had experienced the robust, strong job market of the early part of the decade. Just as suddenly, many of us saw our trainees struggling to find a suitable position in the midpart of the decade and the future was quite uncertain. By the year 2000, considerable uncertainty still remained, despite the fact that our data were showing a return to strength.
In our most recent article, published in the September issue of AJR (Vol. 187:3, pp. 601-602), we found a downtrend in demand: fewer jobs per job seeker and fewer vacancies per program from 2002 to 2004. In 2005, however, the data suggest another increase in demand and an increased shortage of radiologists.
What do these current trends imply and how can we meet these challenges? While the "shortage" of radiologists may not be severe now (it certainly does not compare to 2000 and 2001), the relative growth in volume of our specialty is not being matched by the growth in personnel.
While true productivity growth may be part of the solution (see "How Could the Radiologist Shortage Have Eased?" AJR, September 2006, Vol. 187:3, pp. W249-W254), I believe that much of this perceived productivity growth is actually a lengthening of our workday and workweek. If that is indeed the case, then we will eventually reach the limit of human capability. We may truly find ourselves in short supply of qualified individuals.
What may occur if we do not meet the growing needs of our specialty? First and foremost, our patients may suffer. If we cannot interpret every image or find ourselves interpreting at a pace that is suboptimal, then clinical care may be sacrificed. Furthermore, if we cede control of certain imaging to our lesser-trained clinical colleagues, patient care may also be hurt.
Second, our specialty itself may suffer as further inroads by our clinical colleagues take on speed and momentum, leaving us with a smaller portfolio. We have already seen gynecology and cardiology colleagues take control of certain areas of imaging and intervention. If this were to continue, we could find ourselves representing a small and dwindling percentage of total imaging.
Where are the solutions to this problem? We must separate our short-term fears of oversupplying radiologists from the longer-term issues of permanently being relegated to a niche specialty. We must train more radiologists, and this requires a concerted effort by the leadership of our major societies and the chairs of academic departments. While the U.S. Centers for Medicare and Medicaid Services may not increase its funding of positions, each individual hospital does have latitude to shift resources to diagnostic radiology. Furthermore, one can make a strong argument that positions funded out of clinical revenues (as opposed to extramurally funded) are self-supporting. In addition, other sources (military, Veterans Affairs, etc.) of funding are available to select institutions and applicants. Thus, there is no structural excuse to limit our growth.
We also must engage the physician associate and radiology assistant communities. Grassroots efforts are working, but are slow in achieving the goal of having these practitioners work with us to meet patient care needs.
Our field faces a multitude of threats: reduced reimbursement, self-referral, radiation safety issues, and a heightened awareness by all payors that we are an important component of healthcare costs. But in the face of our recent growth in demand, our supply is woefully inadequate, leaving us quite vulnerable. While some individuals may appreciate the relative shortage because it results in short-term higher salaries and wages, it may be the proverbial battle success in a lost war. We will have failed as a specialty if we allow a shortage of our own making to lead to our diminution. As it takes at least six years from "match day" to train a radiologist, action must happen soon. It is my opinion that this opportunity should not be allowed to slip away. Please let us know your thoughts.
By Dr. Howard P. Forman
AuntMinnie.com contributing writer
November 23, 2006
Forman is an associate editor of health policy for the American Roentgen Ray Society (ARRS). This article originally appeared in the American Journal of Roentgenology (November 2006, Vol. 187:5, pp. 1147-1148). Reprinted by permission of the ARRS.
Related Reading
How to win the coronary CTA turf war, October 9, 2006
MRI and CT imaging: How fast can reimbursement be cut? September 20, 2006
Radiology reimbursement faces major changes, August 21, 2006
Medicare 2006 and beyond: What comes after 'critical'? July 25, 2006
Copyright © 2006 American Roentgen Ray Society














