Hustinx R, Lemaire C, Jerusalem G, Moreau P, Cataldo D, Duysinx B, Aerts J, Fassotte MF, Foidart J, Luxen A.
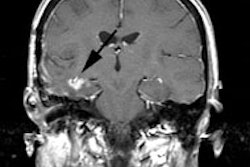
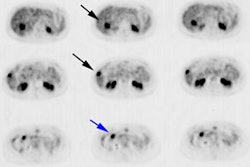
18F-FDG PET imaging is now established as a valuable tool for evaluating cancer patients. However, a limitation of (18)F-FDG is its absence of specificity for tumor. Both protein synthesis and amino acid transport are enhanced in most tumor cells, but their metabolism is less affected in inflammation. We therefore decided to evaluate the ability of PET with 2-(18)F-fluoro-L-tyrosine ((18)F-TYR) to visualize cancer lesions in patients compared with (18)F-FDG PET. METHODS: (18)F-FDG PET and (18)F-TYR PET were performed on 23 patients with histologically proven malignancies (11 non-small cell lung cancers (NSCLCs), 10 lymphomas, and 2 head and neck carcinomas). Fully corrected, whole-body PET studies were obtained on separate days. (18)F-FDG studies were performed after routine clinical fashion. (18)F-TYR studies were started 36 +/- 6 min after tracer injection and a second scan centered over a reference lesion was acquired after completion of the whole-body survey-on average, 87 min after injection. Standardized uptake values (SUVs) were calculated for all abnormal foci and for various normal structures. Results were compared with pathologic or correlative studies. RESULTS: (18)F-FDG PET correctly identified 54 malignant lesions, among which 36 were also visualized with (18)F-TYR (67%). (18)F-TYR did not detect any additional lesion. Tumor SUVs (SUV(bw), 5.2 vs. 2.5), tumor-to-muscle (7.4 vs. 2.7), and tumor-to-mediastinum activity ratios (3 vs. 1.4) were higher with (18)F-FDG than with (18)F-TYR. Two of 11 NSCLCs and 4 of 10 lymphomas were understaged with (18)F-TYR compared with (18)F-FDG. Although the NSCLC lesions missed by (18)F-TYR PET were small, several large lymphoma lesions did not accumulate the tracer. In 4 patients, (18)F-TYR-positive lesions coexisted with (18)F-TYR-negative lesions. There was a high physiologic (18)F-TYR uptake by the pancreas (average SUV(bw), 10.3) and the liver (average SUV(bw), 6.3). Muscle and bone marrow uptakes were also higher with (18)F-TYR than with (18)F-FDG: average SUV(bw), 1 versus 0.7 and 2.6 versus 1.8, respectively. There was no change over time in the (18)F-TYR uptake by the tumors or the normal structures. CONCLUSION: (18)F-TYR PET is not superior to (18)F-FDG PET for staging patients with NSCLC and lymphomas.