The new lesions that sometimes appear on chest radiographs of patients undergoing treatment for tuberculous pleural effusion are typically transient and benign, according to a newly published evaluation.
This paradoxical response to treatment caught the attention of radiologists at Hanyang University hospitals in Seoul and Kuri, South Korea, who decided to do a retrospective analysis of cases. Their findings were published in the August issue of Radiology.
The researchers retrieved the medical records of all 141 patients over age 15 who received chemotherapy for tuberculous pleural effusion and were followed up with chest x-rays at least 12 months during the period of June 1994 to December 1995. Among these were 16 patients (11.3%) who responded to treatment with a decrease of pleural fluid but subsequently developed new lung lesions. Patients who apparently had earlier lesions that were obscured until their effusion cleared were excluded.
Although the originating group of 141 included patients as old as 80, the 16 patients with paradoxical lesions were all between 22 and 33 years of age. Two of the 16 patients had second episodes of paradoxical lesions 5 to 6 months after their first episodes.
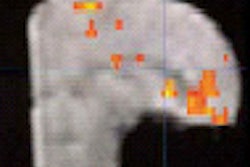
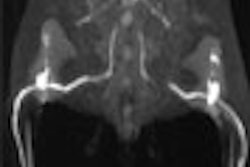
Most of the paradoxical episodes resulted in peripheral pulmonary lesions with a mean peak diameter of 3 cm. All of the lesions had radiographic features of postprimary tuberculosis. In all but one episode, the new lesions were ipsilateral to the side of previous pleural effusion. The radiographic findings were generally followed up by either a CT scan or biopsy. However, the authors suggested the latter evaluation was probably unwarranted given the unlikelihood of malignancies among such young patients (Radiology, August 2002, Vol.224:2, pp. 493-502).
The CT scans showed that none of the lesions had the features of rounded atelactasis that may develop in the wake of pleural effusion. Microbiologic tests excluded the possibility of nontuberculous infection. In addition, the authors found no indication of treatment noncompliance that would explain the lesions, although that possibility could not be entirely ruled out.
All of the patients continued with an unchanged drug regimen after the appearance of their new lesions. After the new lesions reached their maximum diameter, all gradually decreased over 3-18 months before disappearing or leaving residual lesions.
Over the years, the authors wrote, other observers have reported a variety of paradoxical responses to "apparently adequate" antituberculous therapy. These responses included new lesions, development or enlargement of lymph nodes, development of pleural effusion, and progression of pulmonary infiltrates. The paradoxical response typically appears 3-12 weeks after the start of a rapid bactericidal therapy, and usually regresses without a change in treatment.
Among the handful of reports on paradoxical lesion development, one Japanese-language study found a similar incidence of 11.5% with 26 cases out of 226 patients with tuberculous pleural effusion (Kekkaku, May 1994, Vol.69:5, pp. 345-350).
The South Korean authors noted that their more recent evaluation found lesions both in patients with and without active tuberculosis They also found that chest radiographs wouldn’t show parenchymal disease and subpleural tuberculous lesions until they undergo transient worsening, possibly from an immunologic-rebound response to treatment. But even if paradoxical lesions cannot be easily explained, they can be easily handled.
"Results of this study demonstrate that there are patients who develop new pulmonary lesions during medicationfor tuberculous pleural effusion, which implies not failureof the current therapeutic regimen but rather transient worseningof tuberculosis that subsequently disappears with continuationof the same medication," the authors concluded. "It is important to recognize this clinicallyimpressive but benign paradoxical pulmonary response and toavoid unnecessary invasive procedures or changes of currentappropriate therapy."
By Tracie L. Thompson
AuntMinnie.com contributing writer
August 23, 2002
Related Reading
Abnormal chest x-ray may detect infection in patients with asymptomatic HIV disease, May 30, 2002
Copyright © 2002 AuntMinnie.com