The new biologic therapies for rheumatoid arthritis (RA) are causing a shift in treatment goals, according to Dr. Josef Smolen, professor and chair of medicine at Lainz Hospital in Vienna.
"The old approach was to slow disease progression only after RA was clearly evident, and to focus treatment on pain and inflammation," according to Smolen, who spoke at the 2003 European Congress of Rheumatology meeting in Lisbon, Portugal. The new goal should be preventing disease progression, he said.
He and colleagues found that early use of the tumor necrosis factor-α inhibitor (TNF-α) infliximab (Remicade) is associated with a reduction in RA-related disability. In this study, known as the Active Controlled Study of Patients Receiving Infliximab for the Treatment of Rheumatoid Arthritis (ASPIRE), the investigators randomized 1,049 patients with early RA to receive either infliximab combined with methotrexate or methotrexate monotherapy. The study was double-blinded and placebo-controlled. Patients were drawn from North America, Europe, and Israel.
The investigators wanted to see if any of the treatment regimens were associated with sustained improvement in the signs and symptoms of RA by the 54th week of the study. They considered percentage improvement in baseline, expressed by the American College of Rheumatology (ACR) score of at least 20% improvement (ACR-20), and the Health Assessment Questionnaire (HAQ).
At week 54, the percentage of patients with an ACR-20 response was 39% in the 3 mg/kg infliximab combination therapy arm, 47% in the 6 mg/kg infliximab combination arm, and 26% in the methotrexate monotherapy arm. In each of the infliximab arms, 76% of patients had an improvement of at least 0.3 in the HAQ scores, compared to 65% of the methotrexate monotherapy arm and 76% in each of the infliximab arms.
In addition, Smolen said that the study’s radiographic findings indicate that erosive joint destruction occurs early, a finding that suggests patients would benefit from "early aggressive therapy."
These findings show not only the importance of early intervention in RA but also the changing role of radiologists in RA treatment as well as the need for the proper imaging studies, according to Dr. Michael Richardson, a professor of radiology and orthopedics at the University of Washington in Seattle.
"There’s a lot of interest in preventing joint erosions at all in RA," said Richardson, agreeing that early intervention has value. He pointed out that every year, 5% to 10% of people with RA go on disability, and that preventing this development would lessen the burden of disease for patients as well as the broader society.
"The things we see on x-ray, such as swelling of joints and soft tissue and joint-space narrowing, aren’t great findings, because patients already know about it," he said. "The horse is out of the barn when we see it."
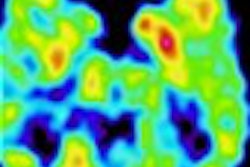
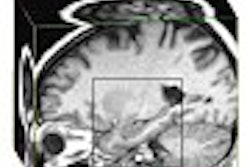
Instead, radiologists need to look for pannus, the inflammatory tissue that forms in the synovium between the joints. "Pannus is not a happy thing for the joint because it causes damage to the cartilage eventually, and then to the joint capsule and to the bone itself," he said. He noted that pannus is present before changes occur in the bone, and is detectable with gadolinium-enhanced MRI.
By Paula MoyerAuntMinnie.com contributing writer
August 18, 2003
Related Reading
Early RA combination therapy offers no long-term advantage, August 13, 2003
Adalimumab improves radiographic outcomes in arthritis, June 20, 2003
Dynamic MRI can discriminate active from inactive rheumatoid arthritis, May 30, 2003
Ultrasonography may be useful in evaluating arthritis treatment, February 5, 2003
Copyright © 2003 AuntMinnie.com