Ultrasound has always been a multiplanar imaging tool -- as long as the patient is lying down. Once the patient leaves the examining table, all that is left are frozen 2D images.
But 3D ultrasound has brought the ability to store, think, and work with volumes. And volume data has brought the ability to work in the multiplanar format even when the patient is not on the examining table.
Four-dimensional ultrasound, which entails simultaneous real-time 3D reconstruction and surface rendering, has played a very important role in fetal imaging. However, recently its role in abdominal imaging has also been recognized in some applications.
Fluid has always been the sonologist's friend, and 3D ultrasound has worked effectively in all fluid-filled structures. The virtual sonographic endoscopic views of the dilated calyceal systems and the urinary bladder have yielded spatial information about intraluminal lesions, their size, and their margins like never before. The presentation of information to the referring physician has also dramatically improved.
 |
| Exquisite 3D reformation showing the dilated calcyceal system on the left and the dilated upper ureter with a calculus on the right. |
A plane of multiplanar imaging that has been most appreciated is the coronal plane, or what is now known as the C-plane. The exquisite anatomical relationships of the prostate and the seminal vesicles are well brought out by the C-plane. The precise anatomy at the verumontanum can also be appreciated in greater detail.
 |
| C-plane view of the prostate showing the region of the verumontanum (arrow). The proximal urethra (arrowhead) is also seen. |
VOCAL is an add-on software application that comes with the package of 3D and 4D ultrasound machines. It can calculate volumes in a more precise manner than the ellipsoidal formula for volumes, which was previously used. VOCAL is precise and easily reproducible, especially with irregular-shaped collections.
 |
| An irregular-shaped perinephric collection showing calculation of volume using the VOCAL software on 3D volume. |
The volume contrast imaging (VCI) for thin-section viewing of structures (in 2-mm, 5-mm, or 10-mm slices) helps enhance the contrast between different planes, picking up subtle differences in margins of lesions or changes in outline.
 |
| VCI images of 4-mm thickness show a small cortical break in the kidney (image on the right) with perinephric hematoma. |
In the urinary bladder, the presence of urine creates a physiological acoustic window to render the urinary bladder wall and the trigone. This helps create virtual cystoscopic views, also known as sonocystoscopic views, of the urinary bladder lumen.
 |
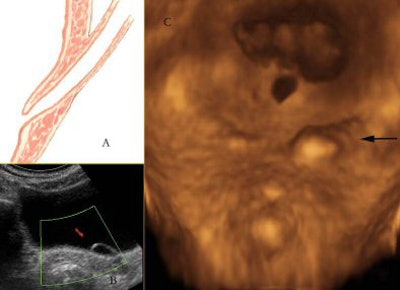
| Three-dimensional rendering of the trigone of the urinary bladder. An anatomical illustration (A) of the intramural course of the terminal ureter gets dilated in some cases to form an ureterocele as seen on 2D scan (B). Three-dimensional rendering (C) shows a sonocystoscopic image of the same (arrow), bringing out the elevated left ureteral ridge secondary to the ureterocele in a lucid manner. |
Small polypoidal lesions in the urinary bladder in the setting of relevant clinical symptoms can be malignant. Three-dimensional ultrasound helps render these small tumors, especially transitional cell carcinoma (TCC) in the urinary bladder, and delineates the surface characteristics in a much better way.
 |
| Small transitional cell carcinoma seen on 2D image (A), and rendered with irregular surface characteristics on the 3D sonocystoscopic image (B). |
Three-dimensional power angio is very helpful in understanding tumoral angiogenesis and differentiating normal and abnormal branching patterns. It can also be used to study the perfusion in a transplant kidney. A transplant kidney, being superficial in location, is amenable to 3D angiographic mode display with ease.
 |
| Three-dimensional ultrasound in angiographic mode shows the vascularity of a transplant kidney. |
Three-dimensional and 4D ultrasound are here to stay. Their uses in abdominal imaging -- especially in the kidney, ureter, and bladder (KUB) region -- are just beginning to be appreciated. With better resolution and faster acquisition speeds in the future, the delineation of anatomy of normal and abnormal lesions is only going to improve.
By Dr Nirvikar Dahiya
AuntMinnieIndia.com contributing writer
January 6, 2005
Dr Nirvikar Dahiya is head of the department of ultrasound imaging at KG Hospital and Post Graduate Institute in Coimbatore.
All images courtesy of and copyrighted by Dr Nirvikar Dahiya, KG Hospital, Coimbatore.
Suggested Reading
- Rankin RN, Fenster A, Downey DB, et al. "Three-dimensional sonographic reconstruction: Techniques and diagnostic applications." AJR 1993;161:695.
- Hamper UM, Trapanotto V, Sheth S, et al." Three-dimensional ultrasound: Preliminary clinical experience." Radiology 1994;191:397.
- Riccabona M, Nelson TR, Pretorius DH, Davidson TE. "In Vivo Three-dimensional sonographic measurement of organ volume: Validation in urinary bladder." J Ultrasound Med 1996;15:627-623.
- Flannigan GM. Editorial: Imaging,stone disease. Curr Opin Urology 1997;7:U10-U12.
- Sakr WA, Grignon DJ, Crissman JD. "Histopathology of transitional cell carcinoma of the urinary bladder." Curr Opin Urology 1997;7:287-292.
- Rasmussen SN, Haase L, Kjeldsen H, et al. "Determination of renal volume by ultrasound scanning." J Clin Ultrasound 1978;6:160.
- Jones TB, Ruddick LR, Harpen MD, et al. "Ultrasonographic determination of renal mass and renal volume." J Ultrasound Med 1983;2:151.
- Grossman H, Rosenberg ER, Bowie JD, et al. "Sonographic diagnosis of renal cystic disease." AJR 1983;140:81.
- Khurana A, Dahiya N. "3D and 4D Ultrasound: A Text and Atlas." Anshan, U.K. 2004.
Copyright © 2005 AuntMinnie.com
















