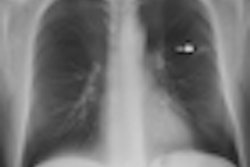
With all the attention being paid to CT lung cancer screening, what about x-ray? Italian researchers believe that radiology's oldest modality could be revived as a screening tool with a technological twist -- digital tomosynthesis. They describe their findings in the June edition of the Journal of Thoracic Oncology.
The utility of x-ray as a lung cancer screening tool has largely been dismissed in several clinical studies, including the 2009 National Lung Screening Trial (NLST), which found that CT had a 20% mortality benefit over screening performed with conventional x-ray.
But digital chest tomosynthesis has the potential to perform better, and it is much cheaper than CT. A group of researchers tested the hypothesis that a population of high-risk former smokers could be screened with tomosynthesis, with suspicious cases sent on to low-dose CT for further workup.
"Although it lacks the depth resolution of CT, tomosynthesis provides some of the benefits of CT at lower costs and radiation dosages," wrote lead author Dr. Alberto Terzi, of S. Croce City Hospital in Cuneo, and colleagues. "Furthermore, digital chest tomosynthesis is less expensive than CT at approximately one-sixths of the cost of a CT" (JTO, June 2013, Vol. 8:6, pp. 685-692).
The researchers enrolled 1,843 subjects who met the following eligibility criteria: 45 to 75 years of age, smoking history of 20 pack-years, and no malignancy for the past five years (NLST and most clinical guidelines use a threshold of 30 pack-years). Of the group, 77% were current smokers. Each patient underwent a tomosynthesis exam as a baseline measure. Patients who had benign nodules or nodules smaller than 5 mm received a second chest tomosynthesis exam a year later.
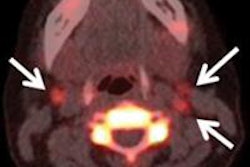
Patients with ambiguous results, nodules larger than 5 mm, or multiple nodules were given a low-dose or contrast-enhanced CT scan after the baseline chest tomosynthesis scan. If the CT exam showed a benign nodule, the patient was asked to return for follow-up CT in three to six months, and then again at 12 months. However, if CT indicated malignancy, the patient underwent a PET scan.
With chest tomosynthesis, Terzi's team found pulmonary abnormalities in 268 patients (14.5%). Of these patients, 132 (7.2%) subsequently had a CT exam, and 68 (4.9%) were referred for follow-up CT. Twenty-seven (1.46%) patients had a PET scan, and lung cancer was detected in 18 (0.98%) of them.
The detection rate of tomosynthesis for all nodules was 18.4%, comparable to the rate reported for low-dose CT, according to the authors.
The study indicates that digital chest tomosynthesis has cost advantages as a first-line screening tool compared to CT alone, Terzi and colleagues wrote. Tomosynthesis could be used to select high-risk individuals who might be suitable for CT screening, rather than simply sending those patients to CT screening right away.