In a face-off of two PET radiopharmaceuticals, FDG-PET/CT outperformed F-18 fluorothymidine (FLT) PET/CT in the diagnosis of postoperative thyroid cancer lymph-node and distant metastases, making the hybrid modality more suitable for examining disease recurrence, according to a study in the June issue of Radiology.
Japanese researchers found that FDG-PET had greater sensitivity, specificity, and accuracy among 20 patients and produced fewer false positives in cervical lymph nodes than FLT-PET.
The study was led by Dr. Masatoyo Nakajo, PhD, from Kagoshima University's Graduate School of Medical and Dental Sciences (Radiology, June 2013, Vol. 267:3, pp. 891-901).
Most common thyroid cancer
Differentiated thyroid cancer is the most common form of the disease. Previous studies have found that the overall survival rate at 10 years after the discovery of distant metastases is only 40%, noted Nakajo and colleagues, and these metastases occur in 10% to 15% of patients. In addition, recurrent cervical disease is associated with increased morbidity and mortality in some high-risk groups.
"Thus, the accurate diagnosis and characterization of nodal and distant metastases is highly important for the management of differentiated thyroid cancer," the authors wrote.
FDG-PET has been used to assess postoperative differentiated thyroid cancer, while FLT-PET has been used to evaluate the cellular activity of several forms of cancer such as colorectal and lung carcinomas.
"To our knowledge, however, the biologic behavior of FLT in thyroid tumors is unknown," Nakajo and colleagues wrote. So the aim of their study was to compare PET/CT performed with FDG and FLT for the diagnosis of metastases from postoperative differentiated thyroid cancer.
The prospective study evaluated 15 women (mean age, 51 years; range, 22 to 79) and five men (mean age, 61 years; range, 52 to 67) between March 2010 and February 2012. Ten patients were enrolled in the study after thyroidectomy and before initial iodine-131 (I-131) therapy for thyroid ablation or metastases. The other 10 patients were enrolled before a second I-131 therapy for recurrence or to confirm the efficacy of initial therapy. Initial or repeat I-131 therapy was performed three to 13 days after PET/CT.
All PET/CT scans were performed on a Discovery STE PET/CT system (GE Healthcare), with image acquisition starting approximately one hour after intravenous injection of 3.7 MBq/kg of FDG. For FLT-PET/CT, image acquisition began approximately one hour after intravenous injection of 3.7 MBq/kg of FLT.
The spiral MDCT scan went from the brain to pelvis immediately before PET, which was performed over the same area. The acquisition time was 2.5 minutes per bed position, with eight bed positions.
Two radiologists visually interpreted the FDG- and FLT-PET/CT images with no knowledge of results at clinical and pathologic follow-up. Images were read independently at random with an interval of four weeks between interpretations.
The scans revealed that 19 patients had papillary carcinoma and one patient had follicular carcinoma. Of the 20 patients, 13 (65%) had concordant uptake of FDG and FLT and seven (35%) had discordant uptake.
FDG outperforms FLT
Patient-based analysis revealed that FDG-PET/CT achieved sensitivity of 92% (12/13 patients), compared with 69% (9/13 patients) for FLT-PET/CT. Specificity was 86% (6/7 patients) with FDG, compared with 29% (2/7 patients) for FLT. FDG had an accuracy of 90% (18/20 patients), compared with 55% for FLT (11/20 patients).
FDG-PET/CT also bested FLT-PET/CT in the lesion-based analysis in diagnosing lymph-node and distant metastases, as shown in the following charts.
| Diagnosis of lymph-node metastases | ||
| FDG-PET/CT | FLT-PET/CT | |
| Sensitivity | 85% (29/34 lesions) | 50% (17/34 lesions) |
| Specificity | 99% (254/246 lesions) | 91% (223/246 lesions) |
| Accuracy | 98% (274/280 lesions) | 86% (240/280 lesions) |
| Diagnosis of distant metastases | ||
| FDG-PET/CT | FLT-PET/CT | |
| Sensitivity | 45% (33/73 lesions) | 7% (5/73 lesions) |
| Specificity | 100% (207/207 lesions) | 100% (207/207 lesions) |
| Accuracy | 86% (240/280 lesions) | 76% (212/280 lesions) |
"The lower sensitivity for distant metastasis may be mainly attributed to the limited resolution of PET for small lung metastases," Nakajo and colleagues noted.
The researchers also found that true-positive lung lesions (mean size, 9.5 mm) were significantly larger than false-negative lesions (mean size, 3.8 mm) with FDG-PET/CT. With FLT, true-positive lung lesions had a mean size of 16 mm and false-negative lesions had a mean size of 5.8 mm.
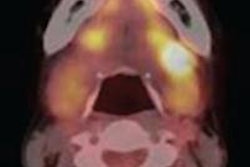
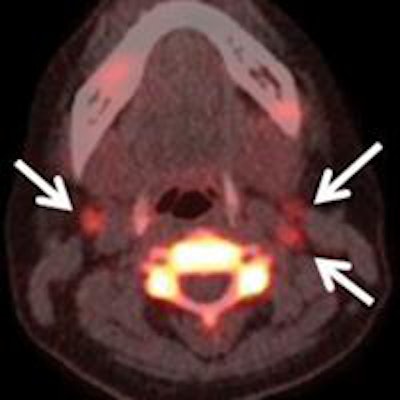
 Images are from a 40-year-old woman with elevated thyroglobulin levels seven months after total thyroidectomy for papillary thyroid cancer. FDG-PET/CT (left) and FLT-PET/CT (right) scans show increased FDG uptake and FLT uptake corresponding to lymph nodes (arrows) in bilateral upper jugular areas. Physiologic increased uptake of FDG is also noted in bilateral sublingual glands (left). Images courtesy of Radiology.
Images are from a 40-year-old woman with elevated thyroglobulin levels seven months after total thyroidectomy for papillary thyroid cancer. FDG-PET/CT (left) and FLT-PET/CT (right) scans show increased FDG uptake and FLT uptake corresponding to lymph nodes (arrows) in bilateral upper jugular areas. Physiologic increased uptake of FDG is also noted in bilateral sublingual glands (left). Images courtesy of Radiology.Nakajo and colleagues cited several limitations to the study, including the relatively small number of subjects and the combination of patients before initial and repeat I-131 therapy. In addition, not all lesions were histologically confirmed, and FDG-PET/CT was used as a standard of reference in conjunction with other clinical factors.
Still, based on the results, the authors concluded that FDG-PET/CT is "superior to FLT-PET/CT in the diagnosis of postoperative differentiated thyroid cancer lymph-node and distant metastases. Thus, FDG-PET/CT is more suitable than FLT-PET/CT for examining recurrence of postoperative differentiated thyroid cancer."