Measurements of muscle mass on dual-energy x-ray absorptiometry (DEXA) can help predict survival in older cardiac surgery patients, according to a study published in the September issue of the American Heart Journal.
Canadian researchers measured muscle mass on DEXA and muscle strength (chair rise test) in patients undergoing heart surgery and found patients with low scores had a three-fold increased risk of mortality after four years. The finding suggests measuring muscle mass provides valuable information for managing high-risk heart surgery patients.
"Lower-extremity muscle strength and [DEXA]-based muscle mass are objective indicators of sarcopenia that are independently predictive of all-cause mortality in older cardiac surgery patients," wrote first author Aayushi Joshi of McGill University, and colleagues.
Studies using CT scans suggest low muscle mass is a potentially important risk factor for adverse outcomes following cardiac surgery. On the other hand, DEXA offers less ionizing radiation at a lower cost than CT, higher accuracy than bioimpedance, and greater accessibility in most hospitals for routine use in bone density evaluation, the authors stated.
Despite this appeal, there has yet to be a study examining DEXA-based muscle mass in the setting of cardiac surgery, according to the authors. In this prospective study, the researchers sought to determine the prevalence and prognostic value of sarcopenia (loss of muscle mass) measured by DEXA and physical performance tests in patients undergoing heart surgery.
The researchers enlisted 141 patients 45 years or older (79% men) referred to Jewish General Hospital in Montreal for coronary artery bypass graft surgery and/or heart valve repair or replacement procedures between February 2013 and January 2017.
Participants were categorized as sarcopenic if they had low appendicular muscle mass on DEXA, defined as greater than 7 kg/m2 for men or greater than 5.5 kg/m2 for women. Low muscle strength was determined by five chair-rise times in 15 seconds or more.
Cox proportional hazards regression was used to test the association between sarcopenia and all-cause mortality over a median follow-up of 4.3 years. The primary outcome was all-cause mortality up to the last available follow-up time ascertained by a combination of medical records, linkage with administrative data sources, and contact with patients or their family members.
The prevalence rates of low muscle mass, slow chair rise time, and sarcopenia (low muscle mass and slow chair rise time) were 24%, 57%, 13%. The four-year survival rate was 79% in the nonsarcopenic group, as compared with 56% in the sarcopenic group.
When sarcopenia was defined as low muscle mass with a cutoff of less than 8 kg/m2 for men and women plus slow chair rise time, the prevalence of sarcopenia was 28%, and it was associated with an adjusted HR of 2.98.
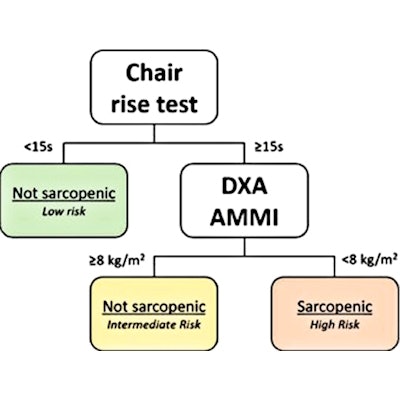
 Classification tree with sarcopenia parameters to predict mortality Modified algorithm to identify sarcopenic patients at increased risk; the Classification and Regression Tree (CART) survival analysis identified the same chair rise cutoff of ≥ 15 seconds but a different Appendicular Muscle Mass Index (AMMI) cutoff of < 8.0 kg/m2 in men and women. Image and caption courtesy of the American Heart Journal.
Classification tree with sarcopenia parameters to predict mortality Modified algorithm to identify sarcopenic patients at increased risk; the Classification and Regression Tree (CART) survival analysis identified the same chair rise cutoff of ≥ 15 seconds but a different Appendicular Muscle Mass Index (AMMI) cutoff of < 8.0 kg/m2 in men and women. Image and caption courtesy of the American Heart Journal."Risk analysis demonstrated sarcopenia was associated with an approximate three-fold increased risk of all-cause mortality among cardiac surgery patients," the researchers wrote.
The researchers suggested a clinical approach based on the results: Start with the chair-rise test to screen for physical frailty and sarcopenia. Patients who complete the test in less than 15 seconds are unlikely to be sarcopenic, while those that cannot may be evaluated further for muscle mass on DEXA.
The authors noted limitations, namely that participants were mostly male -- not unexpected given the higher prevalence of coronary artery disease in men -- and that the study was conducted at a single academic center with one type of DEXA scanner.
"Additional research is needed in multicenter cohorts with larger numbers of female patients to better define the optimal cutoffs ... and to validate the prognostic value with various types of DEXA scanners," the researchers concluded.