A new study from Japan used vascular views in virtual colonoscopy exams to detect blood pooling related to invasive cancers and small vessels of the colorectal wall. Researchers from the National Cancer Center and National Cancer Center Hospital in Tokyo said their technique will improve radiologists' ability to detect not only colonic polyps, but invasive lesions more accurately.
"By means of Hounsfield-transparency settings, we obtained virtual endoluminal images that show vascular structures and delineate invasive cancers of the colorectal walls, called 'vascular views' on contrast-enhanced MDCT colonography (VC)," wrote Drs. Gen Iinuma, Noriyuki Moriyama, Mitsuo Satake, and colleagues in the April American Journal of Roentgenology. "We found that the increase in flow and pooling of blood related to the angiogenesis of cancerous lesions is easy to identify, and that this is useful in the detection of invasive colorectal cancers" (AJR, April 2005, Vol. 184:4, pp. 1194-1198).
The study included 28 consecutive patients (15 men and 13 women, ages 37-77) who presented with 30 invasive colorectal carcinomas detected at conventional colonoscopy. Of these patients, 22 (78.6%) underwent MDCT after a polyethylene-glycol-based bowel prep and preoperative colonoscopy, while the remaining six patients (21.4%), all with advanced colorectal carcinomas, had colonoscopy without the bowel prep. Before treatment the patients also received anticholinergic drugs and room-air insufflation of the bowel, the authors wrote.
Following IV administration of 150 mL iohexol 350 (by power injector at 3 mL/sec) and a 50-second scan delay, virtual colonoscopy images were acquired on a four-slice Aquilion scanner (Toshiba Medical Systems, Tokyo) at 120 kVp, 250-350 mAs, with automatic exposure control, 4 x 2-mm collimation, pitch 5 (pitch factor 1.25).
The images were reconstructed at 1-mm intervals, and transferred to a M900/Pegasus workstation (AMIN, Tokyo) for the creation of 3D images using Hounsfield-transparency settings based on Hounsfield units to show the vascular surface view on a videotape monitor.
"First we adjusted the CT monitor's transparency and opacity setting to a value of 1 to display only the contour of the lumen and the mucosa," the team wrote. "Next, we adjusted the transparency and opacity setting to a value of 2 to display only the arterial-dominant blood with contrast medium. Third, we adjusted the spatial parameters to display only to a depth of 3 mm surrounding the lumen and the mucosa, which corresponds to the thickness of the intestinal wall. Fourth, we overlaid the data displayed in steps one through three to produce a surface and vascular view of the colorectal wall, and then we reduced the surface opacity to produce an obstructed vascular view."
Two radiologists retrospectively reviewed primary lesions, first with a conventional surface view, and then with the vascular view, rendering consensus interpretations rated against all clinical information including colonoscopy; pathological findings and surgically removed specimens served as the gold standard, the authors wrote.
Virtual colonoscopy confirmed all 30 invasive carcinomas, including 18 in the rectum, five in the sigmoid colon, four in the transverse colon, and three in the ascending colon. Twenty-one (70%) of the lesions were larger than 2 cm in diameter. Nineteen (63.3%) were well differentiated and 11 (36.7%) were moderately differentiated at histology. In all, 23/30 (78.7%) lesions were advanced colorectal cancer lesions, and seven (23.3%) were limited to the submucosal layer and therefore defined as early invasive colorectal cancers, the authors wrote. Three of the seven early invasive cancers could be seen on surface endoluminal views, compared to five of the seven that could be identified with vascular imaging.
 |
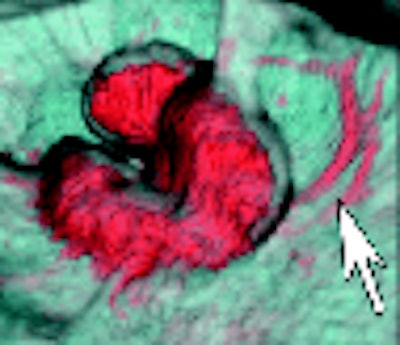
| Above, colonoscopic view and surface and vascular virtual endoluminal images for representative case of advanced colorectal cancer in a 60-year-old woman. Colonoscopic view shows advanced cancer in sigmoid colon. Below, surface virtual endoluminal view in the same patient shows lesion. Bottom, vascular virtual endoluminal image clearly shows blood pooling of tumor and vessels. Iinuma G, Moriyama N, Satake M, Miyakawa K, Tateishi U, Uchiyama N, Akasu T, Fujii T, Kobayashi T, "Vascular Virtual Endoluminal Visualization of Invasive Colorectal Cancer on MDCT Colonography" (AJR 2005; 184:1194-1198). |
 |
 |
"This finding is especially noteworthy because among six advanced colorectal cancer lesions in patients without preparation, four (66.7%) were missed with the conventional surface approach, but all could be visualized on the vascular virtual endoluminal images," Iinuma and colleagues wrote.
Unlike traditional virtual colonoscopy examinations, a bowel prep is not strictly needed because vascular views are unaffected by the presence of stool. Finally, they noted, the introduction of scanners with more detector rows bodes well for further improvements in the technique.
"Vascular views also have a great potential for using blood-flow information to detect small invasive cancers with computer-aided diagnosis, which is expected to improve radiologists' and gastroenterologists' performance enormously" they wrote. "We therefore believe that a focus on the blood supply with the vascular views should be used in conjunction with conventional surface virtual endoluminal images whenever diagnostic or screening contrast-enhanced MDCT is performed until safer contrast media are developed."
By Eric Barnes
AuntMinnie.com staff writer
May 2, 2005
Related Reading
VC with contrast finds more extracolonic trouble, April 11, 2005
Experience sharpens role of IV contrast-enhanced VC, January 19, 2004
Results suggest important new cancer staging role for virtual colonoscopy, December 19, 2003
Virtual colonoscopy techniques evolve with technology, July 25, 2003
Virtual colonoscopy: to contrast, or not to contrast, April 10, 2002
Copyright © 2005 AuntMinnie.com


















